
Dementia: risk factors and prevention
Dementia: risk factors and prevention
Dementia risk can be modified, even in those with increased genetic predisposition.
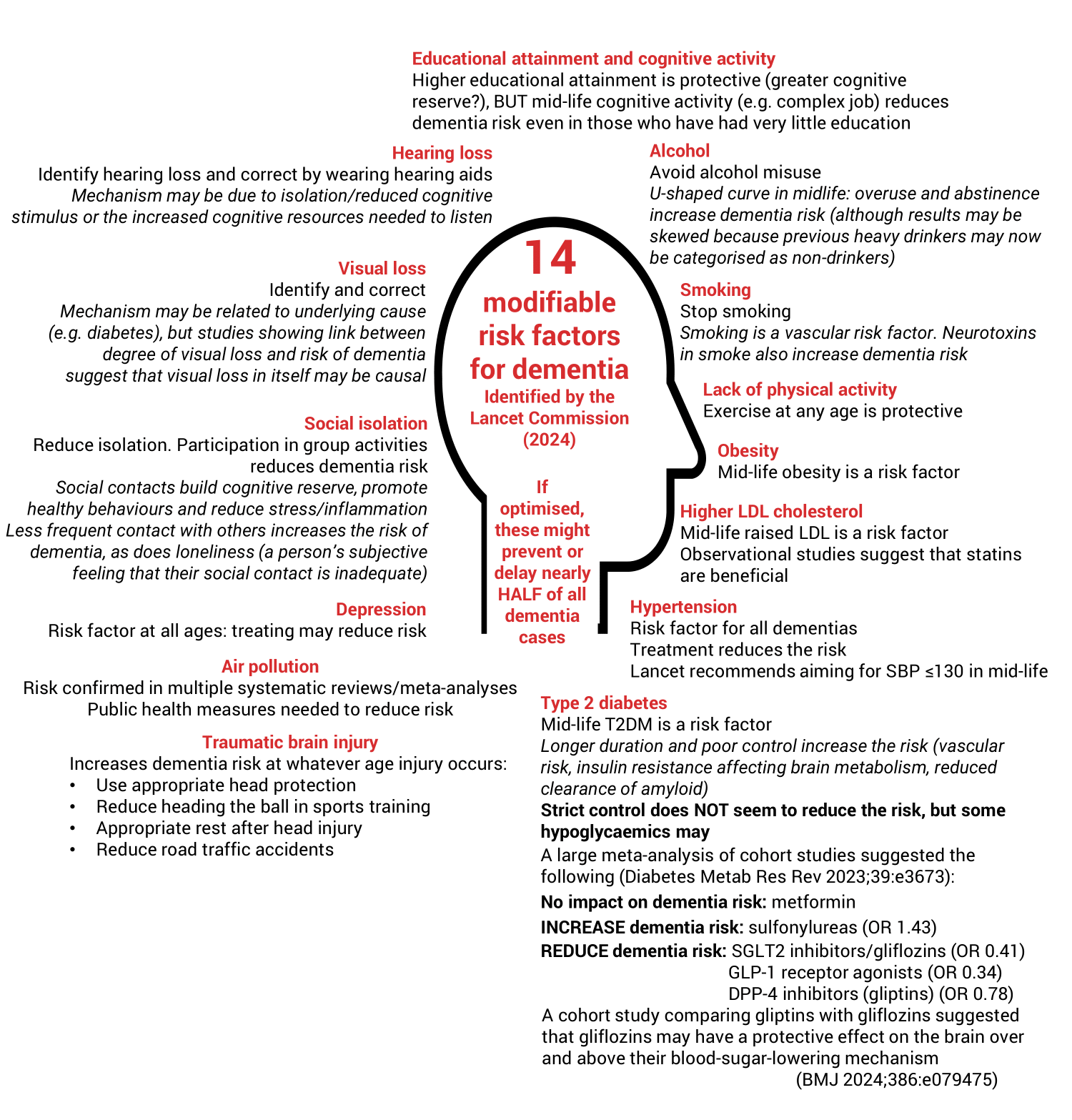
The Lancet Commission on dementia (Lancet 2024;404:572), on which this article is based, lays out 14 modifiable risk factors for dementia. It says that, if optimised, these might prevent or delay nearly half of cases.
This article was updated in October 2025.
Talking to patients about brain health
A qualitative study published in the BJGP found that, while GPs agree that talking to patients about dementia risk should be our role, we almost never explicitly do this (BJGP 2024;74:e242). What's stopping us? The BJGP paper said:
- Time.
- A lack of knowledge about the modifiable risk factors (the rest of this article should help with that!).
- Fear of causing health anxiety by bringing up the term 'dementia'.
The authors suggest that a simple shift, reframing the conversation about ‘dementia risk’ to being about 'brain health', might enable us to bring up this topic more easily.
Modifiable risk factors for dementia
There are the 14 modifiable risk factors identified by the Lancet Commission (Lancet 2024;404:572):
The Lancet Commission identified some further 'potential modifiable risk factors' with insufficient evidence to be included in its core list:
- Sleep: duration and quality of sleep may play a role, with a possible association between sleep apnoea and dementia.
-
Diet: this is likely to be multifactorial, and the Lancet Commission didn’t go into details. However, a BMJ article noted two factors relating to meat consumption (BMJ 2025;388:r126). Having controlled for other risks (smoking, weight, socioeconomics etc.):
- PROCESSED red meat (bacon, sausages, salami, etc.) consumption increases the risk of developing dementia. How great is the risk? One study suggested that in a low consumption group (0.1 servings per day), there might be 8 cases of dementia per 100 people, but in the high consumption group (0.25 servings per day), there would be 9 cases. This risk increase is smaller than that seen in the UK Biobank trial, which showed that every 25g/d of processed meat gave a 44% increase in dementia risk.
- Data on the risk from UNPROCESSED red meat is mixed – one trial has shown an increased risk, but another has shown it to be protective!
- On a positive note, replacing 1 portion of RED meat with a portion of nuts and legumes reduced the risk of dementia by 19%.
- Severe systemic infection (this is separate to specific pathogens known to directly cause dementia, e.g. syphilis, HIV, herpes).
- Psychiatric diagnoses other than depression (which is one of the core modifiable factors), including anxiety, PTSD, schizophrenia and bipolar disorder.
- Multimorbidity and frailty, particularly if chronic illness begins in mid-life.
- Hormone replacement therapy: although the Lancet Commission concluded, “Overall, it is unclear whether menopause and HRT are causally related to dementia risk.” For more on the complex and unclear relationship between HRT and brain health, see our article Menopause, HRT and cognition.
Note that NICE's guideline ‘Dementia, disability and frailty in later life – mid-life approaches to delay or prevent onset’ (NICE 2015, NG16) and the WHO's 'Risk reduction of cognitive decline and dementia’ (2019) explicitly state that there is insufficient evidence to link some of the Lancet Commission's modifiable risk factors, such as depression and hearing loss, to dementia. However, the Lancet Commission is much newer and has looked at much more up-to-date evidence.
Anticholinergics and dementia
The QResearch team (known for the QRisk and QDiabetes tools) has looked at the link between exposure to anticholinergic drugs and risk of dementia (JAMA 2019:179(8):1084). In a UK primary care-based, case-controlled study, it found that there was a strong link between exposure to commonly-used anticholinergic medications and risk of dementia. This was more pronounced for vascular dementia than Alzheimer’s disease.
It is important to note this was an association only – these results do not prove causation! However, the authors do speculate that if causation could be proven, it would mean that approximately 10% of all dementia diagnoses would be secondary to use of these drugs. (See our article Anticholinergic burden scale for more detail.)
Pre-eclampsia and dementia risk
Pre-eclampsia may increase the risk of dementia, but only by a small amount (large Danish cohort study (BMJ 2018;363:k4109)):
- Vascular dementia (hazard ratio 3.46 (CI 1.97–6.10)).
- Alzheimer’s disease (hazard ratio 1.45 (CI 1.05–1.99)).
- Other/unspecified dementia (hazard ratio 1.40 (CI 1.08–1.83)).
There is little women can do to change this and the risk increase is small. Remember, this is cohort data and so shows an association, not causation.
Vitamin D and dementia risk
A large Australian study of healthy older adults (without vitamin D deficiency) looked at the benefits of vitamin D supplementation on the risk of dementia (among other things). It found no evidence to support routine vitamin D supplementation in healthy older adults to prevent cognitive decline (DTB 2025;61:163). You can find more detail on this study in our article on Vitamin D.
Smell and mortality
A study followed 2500 older adults over 12 years, looking at their ability to smell and what happened to them (JAMA Otolaryngo Head Neck Surg 2025:151:558). A standardised test (Sniffin’stick Odour Identification test) was used to assess sense of smell, including the ability to smell things such as garlic, coffee and lemon.
Compared with those with normal smell, those who had poor smell at the start of the study:
- Were much more likely to die during the follow-up period than those with normal smell (6% increased risk of all-cause mortality after 6y follow-up and 5% increased risk of all-cause mortality at 12y follow-up).
- Were much more likely to develop neurodegenerative conditions (including dementia) (23% of all-cause mortality at 6y follow-up was due to dementia). The authors also noted a correlation between carrying one of the genes for Alzheimer’s (APOE protein variant) and losing your smell.
- Were more likely to be frail or malnourished at the 6y follow-up point.
The editorial accompanying the article suggested that more research is needed, but that smell might one day be used as a screening test for future health. For now, the focus should be on recognising that declining smell in older age is a marker of overall poorer health (JAMA Otolaryngo Head Neck Surg 2025:333;1942).
|
Dementia risk factors and prevention
|
This information is for use by clinicians for individual educational purposes, and should be used only within the context of the scope of your personal practice. It should not be shared or used for commercial purposes. If you wish to use our content for group or commercial purposes, you must contact us at sales@red-whale.co.uk to discuss licensing, otherwise you may be infringing our intellectual property rights.
Although we make reasonable efforts to update and check the information in our content is accurate at the date of publication or presentation, we make no representations, warranties or guarantees, whether express or implied, that the information in our products is accurate, complete or up to date.
This content is, of necessity, of a brief and general nature, and this should not replace your own good clinical judgment or be regarded as a substitute for taking professional advice in appropriate circumstances. In particular, check drug doses, side effects and interactions with the British National Formulary. Save insofar as any such liability cannot be excluded at law, we do not accept any liability for loss of any type caused by reliance on the information in these pages.
Here is the link to our terms of use.