 Bacterial meningitis and meningococcal disease
Bacterial meningitis and meningococcal disease
-
1. Bacterial meningitis and meningococcal disease
- 1.1 NICE guidance on bacterial meningitis and meningococcal disease
- 1.2 Bacterial meningitis and meningococcal disease overview
- 1.3 Strongly-suspected meningococcal disease
- 1.4 Strongly-suspected bacterial meningitis
- 1.5 Recognising bacterial meningitis and meningococcal disease
- 1.6 Risk factors for bacterial meningitis and meningococcal disease
- 1.7 Symptoms and signs of bacterial meningitis and meningococcal disease
- 1.8 Extra tips for recognising bacterial meningitis and meningococcal disease
- 1.9 What is the rationale behind the guidance on prehospital antibiotics?
- 1.10 Safety-netting
- 1.11 Should EVERY child with petechiae be admitted?
- 1.12 Long-term outcomes following bacterial meningitis and meningococcal disease
- 1.13 Prior antibiotics and risk of meningitis
This Pearl is provided as free content. Here is the link to our terms of use
Bacterial meningitis and meningococcal disease
Bacterial meningitis and meningococcal disease
Meningitis strikes fear into the heart of parents and clinicians alike. Fortunately, it is something we don’t see very often, but this means our knowledge must far outweigh our experience.
This article was reviewed in June 2024.
NICE guidance on bacterial meningitis and meningococcal disease
Please follow the link for a PDF version of the GEMS for download/printing: Bacterial meningitis and meningococcal disease: GEMS
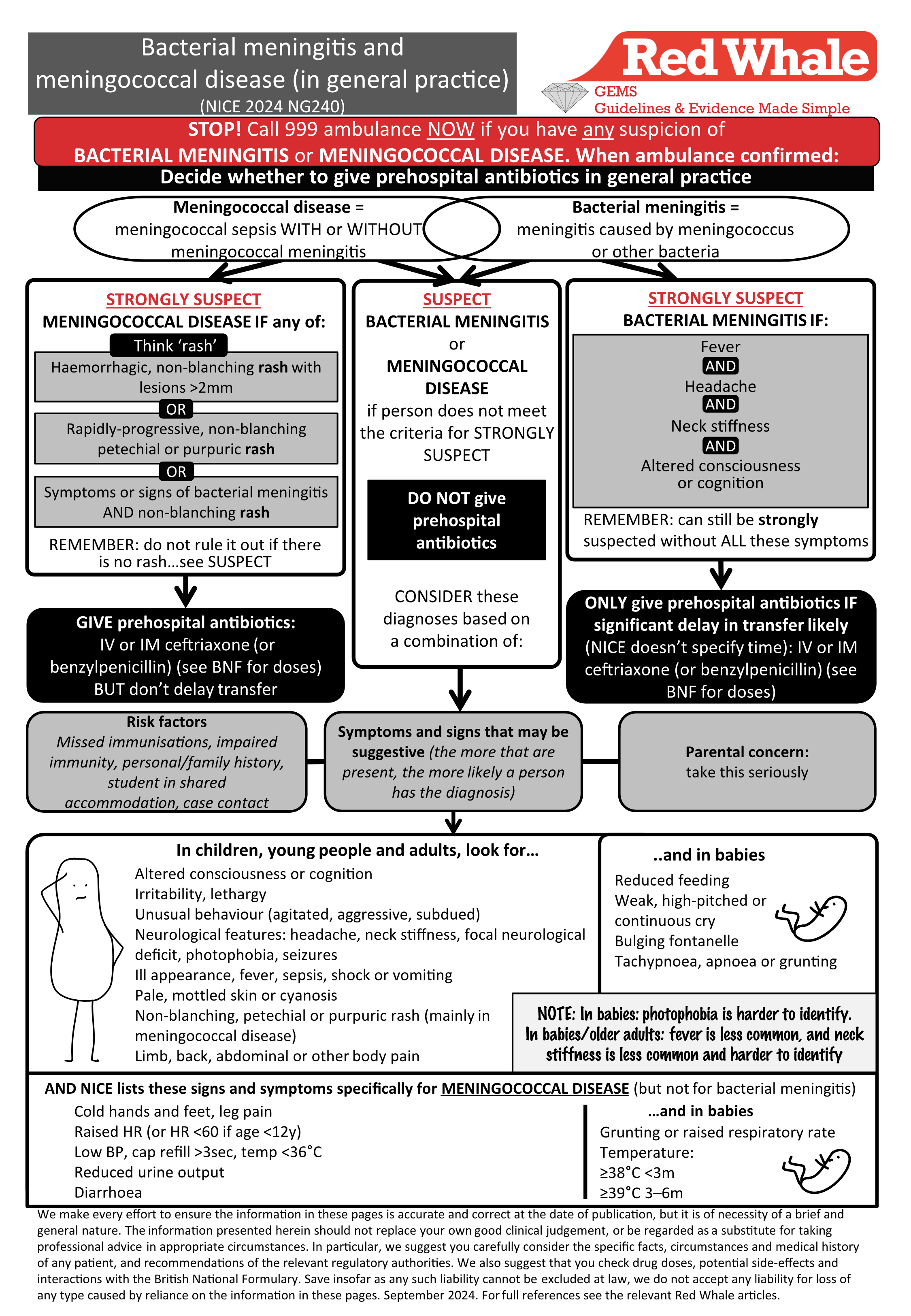
Bacterial meningitis and meningococcal disease overview
The NICE guidance (NICE 2024, NG240) clearly distinguishes between bacterial meningitis and meningococcal disease, although, of course, the two overlap. The guidance for bacterial meningitis includes meningococcal meningitis and meningitis caused by other bacteria. The guidance for meningococcal disease covers meningococcal sepsis, both with and without meningitis.
Bacterial meningitis = meningococcal meningitis OR meningitis caused by another bacteria.
Meningococcal disease = meningococcal sepsis with OR without meningococcal meningitis.
A Lancet article looking at trends in bacterial meningitis in England from 2012 to 2019 reminds us that (Lancet, 2023;32:100692):
- Bacterial meningitis is still an important cause of death in the UK, with an overall case fatality rate of 10%.
- Since the introduction of H. influenzae b, group B & C meningococcus and pneumococcal vaccinations, bacterial meningitis and meningococcal disease rates have fallen dramatically.
- The most common pathogens for bacterial meningitis are N. meningitidis (3m–14y) and S. pneumoniae (≥15y).
- Serogroup B meningococcus is the cause of most cases of invasive meningococcal disease (UKHSA 2024).
- Prior to the vaccination programme, up to 20% of children presenting with fever and a non-blanching rash would have invasive meningococcal disease. Now, this figure is closer to 1%. Hib meningitis is also now rare (Lancet Infect Dis 2021;21:569).
- Bacterial meningitis and meningococcal disease are notifiable diseases in the UK.
What’s new in the 2024 NICE guideline?
In 2024, NICE completely rewrote its guideline on bacterial meningitis and meningococcal disease (NICE 2024, NG240).
NICE bases its guidance on how strongly we suspect bacterial meningitis or meningococcal disease. It divides the guidance into those with ‘strongly-suspected’ meningococcal disease or ‘strongly-suspected’ bacterial meningitis, and then those with simply ‘suspected’ meningococcal disease or bacterial meningitis.
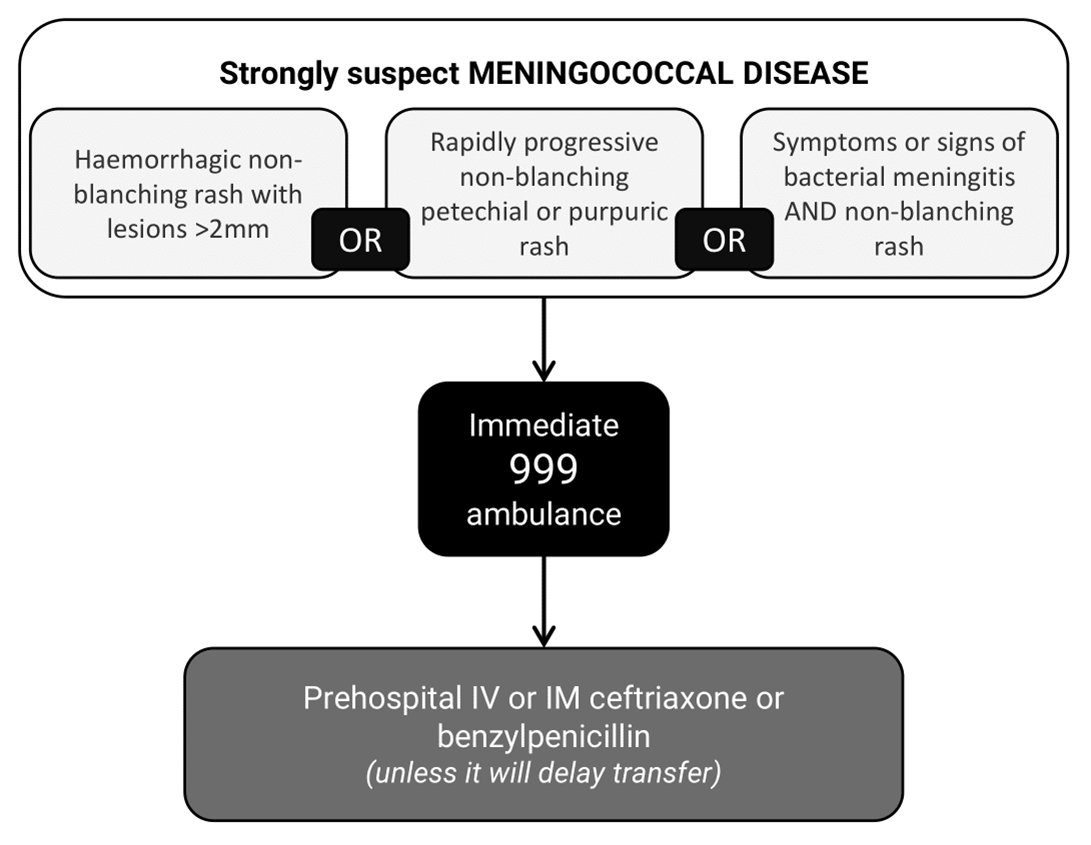
Strongly-suspected meningococcal disease
First, let’s consider ‘strongly-suspected’ meningococcal disease.
NICE states that the RED FLAG SYMPTOMS for ‘strongly-suspected’ meningococcal disease are:
- Haemorrhagic, non-blanching rash with lesions >2mm OR
- Non-blanching petechial or purpuric rash OR
- Symptoms and signs of bacterial meningitis with a non-blanching rash.
Any of these RED FLAG SYMPTOMS warrants an immediate 999 ambulance and prehospital antibiotics (unless it will delay transfer).
Further drug information, including antibiotic doses, is listed in our article Drugs for the GP bag. Always check drug doses in the BNF or BNFc.
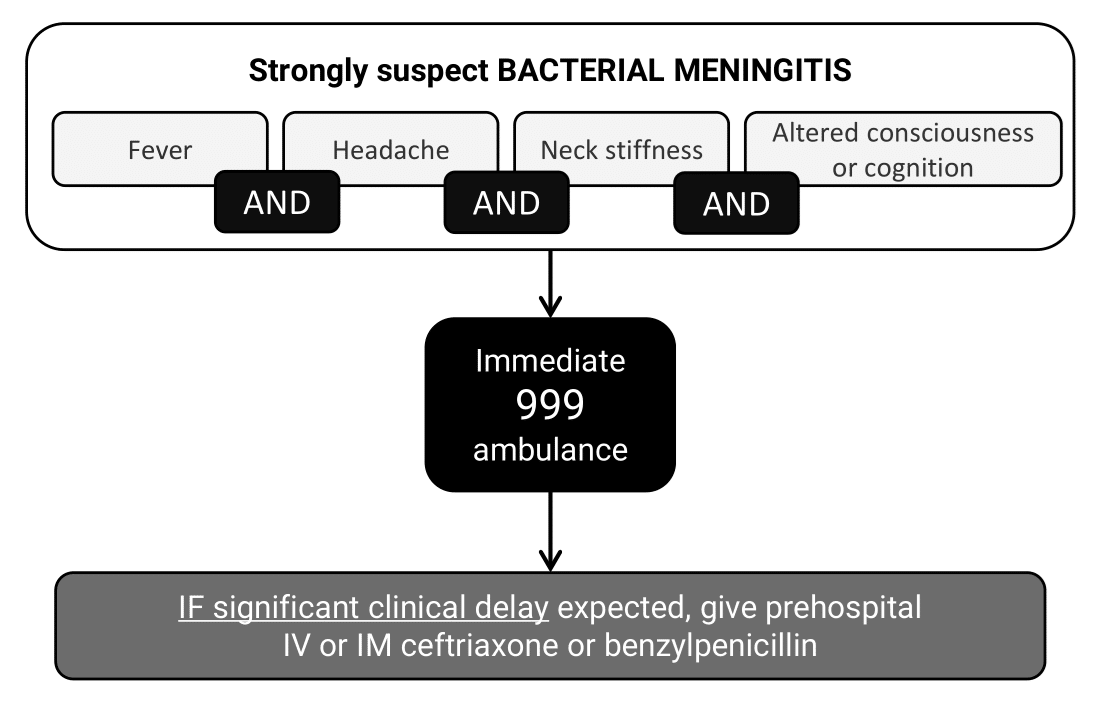
Strongly-suspected bacterial meningitis
Now, let’s consider ‘strongly-suspected’ bacterial meningitis:
In its guidance, NICE is very clear about the RED FLAG COMBINATION for bacterial meningitis:
- Fever AND
- Headache AND
- Neck stiffness AND
- Altered consciousness or cognition.
This combination is mentioned seventeen times (yes, 17). I guess this is something NICE really wants us to remember!
A person with ALL the symptoms in the red flag combination is highly likely to have bacterial meningitis, and warrants an immediate 999 ambulance. Prehospital antibiotics are only given when a significant clinical delay in transfer is expected. Annoyingly, NICE doesn’t say what constitutes a clinically significant delay, but this is a deliberate omission due to lack of evidence.
Further drug information, including antibiotic doses, is listed in our article Drugs for the GP bag. Always check drug doses in the BNF or BNFc.
Recognising bacterial meningitis and meningococcal disease
NICE talks about:
- Strongly-suspected meningococcal disease and strongly-suspected bacterial meningitis, AND THEN
- Suspected bacterial meningitis and suspected meningococcal disease.
Both need transfer to hospital. The key difference is that those with suspected disease are not considered for immediate prehospital antibiotics.
| Disease | Action | Antibiotic |
| Strongly-suspected meningococcal disease |
Immediate 999 ambulance |
Immediate, unless it will delay transfer |
| Strongly-suspected bacterial meningitis | Only if significant delay expected | |
| Suspected meningococcal disease | No | |
| Suspected bacterial meningitis | No |
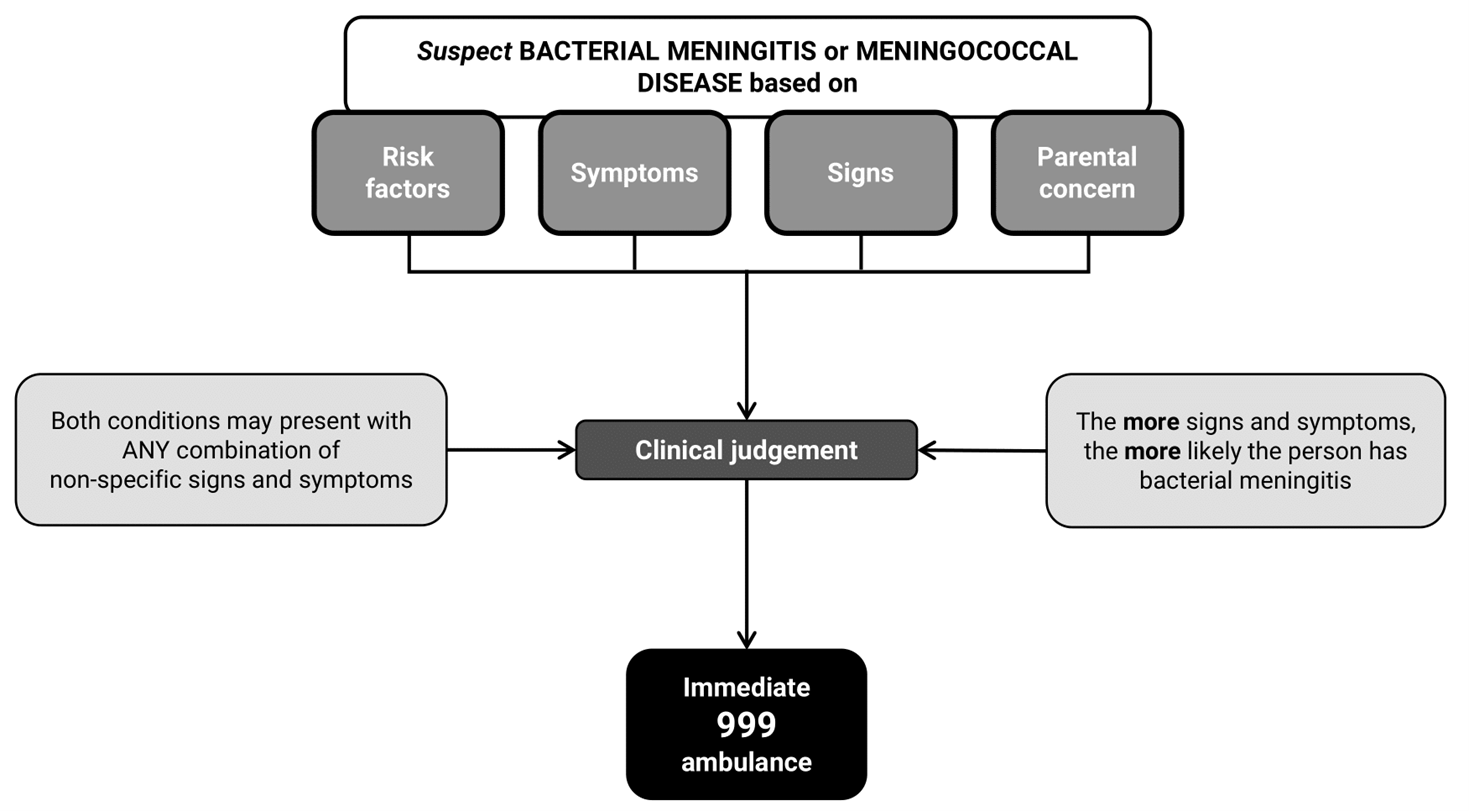
NICE is clear about when to diagnose ‘strongly-suspected’ disease using the red flag symptoms for meningococcal disease or the red flag combination for bacterial meningitis, but what about the less certain ‘suspected’ versions? Here, NICE asks us to use our clinical judgement, based on risk factors, symptoms and signs. We should also take into account parental concern…..AND, just to muddy the waters…
NICE cautions that bacterial meningitis can still be strongly suspected even in those WITHOUT the red flag symptoms, particularly in young babies and older adults.
At Red Whale, we think this means that if you are unsure whether someone has ‘suspected’ or ‘strongly-suspected’ bacterial meningitis, treat them as ‘strongly-suspected’ bacterial meningitis. The priority in both situations is immediate 999 ambulance transfer to hospital.
Risk factors for bacterial meningitis and meningococcal disease
Which risk factors should we consider when thinking about suspected bacterial meningitis or meningococcal disease?
Be particularly alert to bacterial meningitis and meningococcal disease in anyone with the following risk factors:
Missed relevant immunisations:
- Meningococcal.
- Haemophilus influenzae type b (Hib).
- Pneumococcal.
Impaired immune system:
- Reduced or absent spleen function.
- Complement deficiency or inhibition.
History of meningitis:
- Personal history of bacterial meningitis or meningococcal disease.
- Family history of meningococcal disease.
Other:
- Student in higher/further education, particularly if in large, shared accommodation.
- Contact with someone with Hib disease or meningococcal disease, or in an area with an outbreak of meningococcal disease.
For bacterial meningitis (but NOT a risk for meningococcal disease)
- Cochlear implant.
- Cerebrospinal fluid leak.
Symptoms and signs of bacterial meningitis and meningococcal disease
NICE mentions the following symptoms and signs that may be present in bacterial meningitis and/or meningococcal disease:
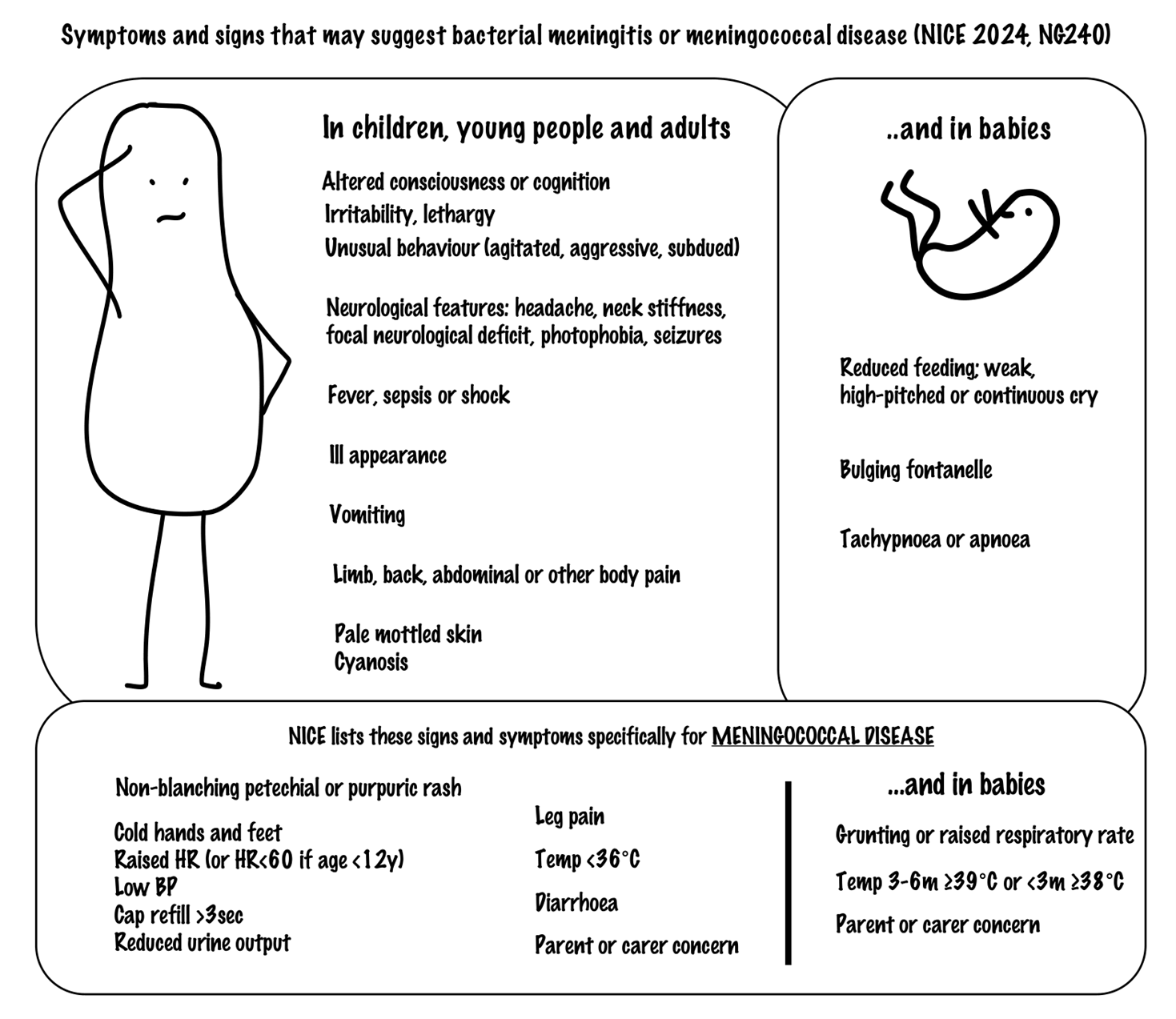
The guidance incorporates some non-specific symptoms and signs such as leg pain and cold hands and feet. These were included in the previous guidance and are based on a qualitative study of 450 children admitted to hospital with meningococcal disease. Retrospective analysis collated the symptoms and signs that parents noted prior to admission (Lancet 2006;367:397).
Many children with meningococcal disease had only non-specific symptoms and signs in the first 4–6h, but most were close to death within 24h, highlighting the rapid progression of the disease and the difficulty in diagnosing it at an early stage. The classic symptoms and signs (non-blanching petechial/purpuric rash, meningism and impaired consciousness) presented late, with median onset of 13–22h.
Importantly, however, there were some early symptoms and signs:
- At a median time of 8h, 72% had developed early symptoms and signs of sepsis:
- Leg pains.
- Cold hands and feet.
- Abnormal skin colour.
- 76% of parents had noticed one of the early symptoms and signs prior to admission.
We should remember to ask about leg pains, cold hands and feet, and abnormal skin colour, and educate parents about these in addition to the ‘classic’ symptoms and signs.
Extra tips for recognising bacterial meningitis and meningococcal disease
When thinking ‘could it be bacterial meningitis or meningococcal disease?’, consider the following:
- These are rapidly-evolving conditions. A person can go from well to moribund within hours. Most deaths from meningococcal disease occur within the first 24h.
- Meningitis AND sepsis can occur together, especially in those with a rash, but meningococcal disease can occur WITHOUT a rash.
Bacterial meningitis and meningococcal disease can be easily missed because:
- Young people and young adults may appear well at presentation, making it difficult to pick up.
- Antipyretics may mask fever. Ask if they have been used.
- Altered level of consciousness, cognition or behaviour in young people and young adults may be put down to alcohol or substance misuse, or, in older adults, dementia or delirium.
- It may be hard to differentiate from other serious infections, e.g. pneumonia, other forms of sepsis, non-bacterial meningitis or intracranial bleed.
- Symptoms such as headache and neck stiffness might not be reported in those with communication difficulties or cognitive impairment, and neck stiffness is less common and harder to identify in babies and older adults.
- The rash can be difficult to see in brown, black or tanned skin. In all skin types, check the whole body for a rash, including nappy area and conjunctivae.
If in doubt, arrange immediate transfer to hospital via 999 ambulance.
What is the rationale behind the guidance on prehospital antibiotics?
NICE is clear that the priority for suspected bacterial meningitis and meningococcal disease is emergency transfer to hospital for urgent testing and treatment.
It found evidence showing no clear benefit to giving antibiotics prior to hospital transfer for bacterial meningitis in terms of all-cause mortality and long-term function, and evidence did not show a clear benefit for prehospital antibiotics in meningococcal disease.
Prehospital antibiotics may affect blood and lumbar puncture test results.
However, given the rapid progression of meningococcal disease, the NICE committee agreed that prehospital antibiotics should be given for strongly-suspected meningococcal disease, but only if this will not delay transfer, and for strongly-suspected bacterial meningitis if a clinically significant delay in transfer is likely.
Which antibiotic should we use?
Ceftriaxone is preferred because it is the more active agent, but benzylpenicillin is included as an alternative when ceftriaxone is not available.
Further drug information, including antibiotic doses, is listed in our article Drugs for the GP bag. Always check drug doses in the BNF or BNFc.
Safety-netting
After your assessment, you may decide it is appropriate to send a person home: for example, a child with a fever and a blanching rash for several days who does not appear ill. If you send a person home after assessment for possible bacterial meningitis or meningococcal disease, safety-net carefully. NICE doesn’t give any specific details here, but reminds us:
- A rash can change from blanching to non-blanching, in which case they should return for reassessment.
- Ask them to return if they develop new symptoms or worsening of existing symptoms.
Should EVERY child with petechiae be admitted?
We have all seen the occasional well child with a non-spreading petechial rash, e.g. in an SVC distribution following retching/vigorous coughing fits. What do we do?
The guidance is clear that a petechial rash is only a red flag for meningococcal disease when it is rapidly progressive or spreading, and, reassuringly, the PiC study determined that only 1% of children presenting to emergency departments with petechial rash and fever had meningococcal disease (Lancet Infect Dis 2021;21:569).
A helpful BMJ review on management of petechiae and purpura in primary care offers some guidance (BMJ 2016;352:i1285). It suggests:
- In a well child, arrange same-day FBC and clotting. If this cannot be done in primary care, you may need to refer to secondary care.
- In a well adult, arrange FBC and clotting within 48h.
This is a situation that requires careful clinical judgement, safety-netting and appropriate reassessment. In the absence of ANY high-risk features, and no fever/history of fever and no symptoms or signs suggestive of serious illness, we may choose to assess and monitor in primary care. The same applies where there is a good explanation for the presence of petechiae in an otherwise well person, e.g. coughing, vomiting or physical causes. If a person is not admitted, specific safety-netting and early reassessment will be necessary. For a diagnostic approach to petechiae and purpura, see our related article Purpura and petechiae: assessment.
Long-term outcomes following bacterial meningitis and meningococcal disease
Bacterial meningitis and meningococcal disease are associated with a number of long-term sequelae, including neurodevelopmental, cognitive, psychological, educational, hearing, orthopaedic, skin and renal problems. Follow-up will be coordinated by secondary care, and includes:
- Audiology assessment within 4w of being well enough for testing.
- Neurodevelopmental assessment and paediatric review for babies, children and young people for up to 2y following discharge. Educational support may be needed.
- Cognitive and psychological support if needed.
- Orthopaedic and skin review if needed, e.g. following amputation or skin necrosis in meningococcal disease.
Beyond this, we should be alert to long-term neurodevelopmental concerns in babies and children, including:
- Problems with learning and increased learning needs. These may come to light when starting nursery or school.
- Negative effects on educational outcomes.
Prior antibiotics and risk of meningitis
The specific reasons why some people get meningitis while most do not remain unclear.
A large BJGP retrospective case–control database study looked at whether prior prescription of antibiotics increased the subsequent risk of meningitis in the following year (BJGP 2016;66:e228). This study included all ages, and both viral and bacterial meningitis.
It found that:
- Patients who had had 4 or more courses of antibiotics in the preceding year were at significantly increased risk of both bacterial and viral meningitis (adjusted OR 2.85 (CI 2.44–3.34)) compared with matched controls.
- There was also a strong association with an antibiotic being issued in the 7d before a meningitis diagnosis (probably reflecting prodromal symptoms).
- There did not appear to be a difference between narrow or broad-spectrum antibiotics.
The authors hypothesised that antibiotics may lower the threshold for subsequent infection by altering the patient’s microbiome, although acknowledged that the lack of difference in narrow and broad-spectrum antibiotics, and the fact an impact is seen for 12m, do not support this. An alternative explanation is that these patients are just more susceptible to infection. Remember: this is an observational study, and causation cannot be determined!
|
NICE on bacterial meningitis and meningococcal disease Diagnosis:
Long-term care:
|
|
|
Are all clinical staff at your practice trained and up to date in recognising the signs and symptoms of bacterial meningitis and meningococcal disease? Do you stock ceftriaxone for emergency use? Do you have an emergency drug box with ceftriaxone and benzylpenicillin, and the doses by weight for different age groups? Do you know where to find it? |
|
|
Useful resources: Websites (all resources are hyperlinked for ease of use in Red Whale Knowledge) |
This information is for use by clinicians for individual educational purposes, and should be used only within the context of the scope of your personal practice. It should not be shared or used for commercial purposes. If you wish to use our content for group or commercial purposes, you must contact us at sales@red-whale.co.uk to discuss licensing, otherwise you may be infringing our intellectual property rights.
Although we make reasonable efforts to update and check the information in our content is accurate at the date of publication or presentation, we make no representations, warranties or guarantees, whether express or implied, that the information in our products is accurate, complete or up to date.
This content is, of necessity, of a brief and general nature, and this should not replace your own good clinical judgment or be regarded as a substitute for taking professional advice in appropriate circumstances. In particular, check drug doses, side effects and interactions with the British National Formulary. Save insofar as any such liability cannot be excluded at law, we do not accept any liability for loss of any type caused by reliance on the information in these pages.
Here is the link to our terms of use.