 Burnout in health professionals
Burnout in health professionals
-
1. Burnout in health professionals
- 1.1 What is burnout?
- 1.2 How common is burnout?
- 1.3 What causes burnout?
- 1.4 The impact of burnout
- 1.5 Spotting burnout in ourselves and our colleagues
- 1.6 What can we do to tackle burnout?
- 1.7 Primary prevention of burnout
- 1.8 Secondary prevention: improving support for individuals and teams
- 1.9 Recovery and rehabilitation after burnout
- 1.10 Personal microskills for preventing burnout
- 1.11 A final thought…
This Pearl is provided as free content. Here is the link to our terms of use
Burnout in health professionals
Burnout in health professionals
|
If you're finding things difficult today, please don’t face it alone. Reach out to a friend, a trusted colleague, your GP or one of the support organisations listed in this article. Support is available – and asking for help is a vital first step. |
Burnout in health professionals is a hugely important issue, affecting both personal wellbeing and patient care. Long hours, high demands, inadequate support and working under increasingly difficult conditions within an NHS system that is under significant strain can leave many clinicians feeling overwhelmed and exhausted.
Burnout is associated with many negative outcomes, including (BMJ 2022;378:e070442, BMJ 2022;378:o2157):
- Poorer patient care, more clinical errors and lower patient satisfaction.
- Reduced professional engagement, loss of commitment and high staff turnover.
- Increased absenteeism.
- Worsening mental and physical health.
So, it's vital that we take this problem seriously. This article explores what burnout is, how to recognise it in ourselves and our colleagues, and some organisational and personal strategies that can help prevent and treat it.
You may also wish to see our related articles: Roadmap to wellbeing: microskills for positive change, Building resilience and Communicating our needs and setting boundaries.
This article was updated in September 2025.
What is burnout?
Burnout is a state of emotional, physical and mental exhaustion caused by excessive and prolonged stress. It is categorised as a syndrome caused by chronic, unmanaged workplace stress, rather than as a medical condition (ICD-11 - World Health Organisation, 2022). However, individuals who are burned out are also at greater risk of mental health problems such as depression, anxiety and suicidality (Front Public Health 2023; 11:1133484).
There are 3 main features of burnout (World Psychiatry 2016; 15:103):
- Exhaustion and fatigue: we feel overextended and drained of physical and emotional energy.
- Reduced sense of accomplishment and professional efficacy: we begin to doubt our skills, feel ineffective and unmotivated, and worry that our work performance is suffering. If burnout isn’t recognised and treated, these feelings can become reality.
- Depersonalisation: we may feel increasingly detached or negative towards patients, colleagues or our work. This can lead to irritability, reduced empathy and a more mechanical approach to patient care, all of which contribute to decreased professional fulfilment.
The impact of burnout in health settings may be underestimated
The impact of burnout in health professionals may be underestimated because clinicians typically strive to complete essential clinical tasks even when exhausted. Those experiencing burnout often adopt ‘performance protection’ strategies that maintain high-priority clinical tasks, while neglecting lower-priority tasks, including interpersonal skills such as reassuring patients (Front Psychiatry 2022; 13:818393).
Compassion fatigue
Compassion fatigue can be an early warning sign of burnout. It can show up as a growing sense of emotional disconnection from patients or colleagues. This response typically develops after prolonged exposure to other people’s pain – whether through witnessing trauma or supporting multiple patients with complex emotional needs.
As a coping mechanism, the mind may begin to create emotional distance. This disengagement can lead to a loss of empathy or a sense of indifference. While this reaction may feel protective at first, it is also distressing because it separates us from others and doesn’t align with our values or how we want to be at work. It also makes it harder to provide compassionate care and function well in our roles (Healthcare 2024; 12:171, Burnout free working 2025; JKP).
How common is burnout?
The 2024 NHS staff survey highlights burnout as a significant concern:
- 30% of staff reported that they felt burnt out because of their work.
- 34% said that work is emotionally exhausting.
- 42% felt worn out at the end of their working day or shift.
- 29% said that they do not have enough time for family and friends during leisure time.
Here are some more statistics showing how burnout affects different groups of health professionals:
| Doctors |
|
| Nurses |
|
| Dentists |
|
| Society of Occupational Medicine 2018, What could make a difference to the mental health of UK doctors?; BJGP 2022; 72:e316; Society of Occupational Medicine 2020, Mental Health and Wellbeing of Nurses and Midwives in the UK; GDC 2021 - a welcome mental health and wellbeing review by the GDC | |
What causes burnout?
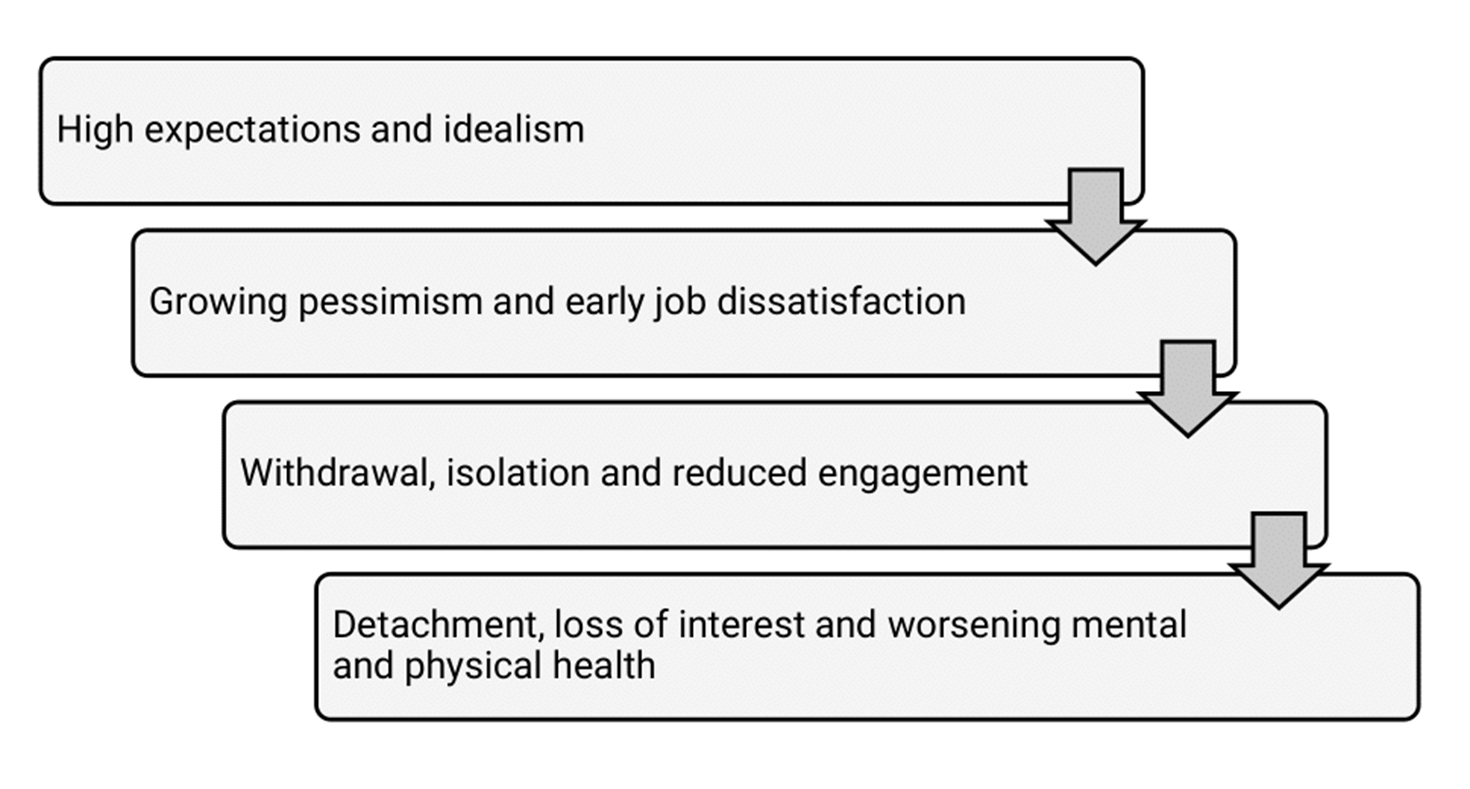
One model of burnout views it as a sequential process that develops in stages across a clinician’s career. Most clinicians start out with enthusiasm and a desire to help others. However, heavy workloads, endless paperwork and overwhelming responsibility – often with little autonomy or control over our working lives – can cause work-related stress. While short-term stress is a natural response that can boost our energy and focus to help meet challenges, chronic and unmanaged stress can take a heavy toll on our wellbeing and may eventually lead to burnout (Society of Occupational Medicine, 2023; Burnout in Healthcare):
Multiple factors are associated with the development of burnout
Rather than a linear pathway, burnout may be better understood as a complex interplay of factors, including workplace conditions, personal resilience and coping strategies (Society of Occupational Medicine, 2023):
| Organisational factors | Individual factors |
|
|
Factors that can make clinician burnout more likely
When we look at the factors above in the context of clinician burnout, we can see how personality traits and behavioural patterns can also increase the risk of burnout in this group:
| Lack of work–life balance | Poor work–life balance makes it harder to prioritise important life areas such as exercise, social activities and hobbies. Clinicians in training, parents of young children and those without support may be especially vulnerable. Long hours and job pressures can leave little time for personal life, while the emotional demands of the job make it hard to switch off, leading to rumination, worry, sleep problems and strained personal relationships. See our article Communicating our needs and setting boundaries for more on this. |
| Rescuer syndrome | This is a personality trait often seen in health professionals; it involves high levels of empathy combined with a strong sense of responsibility. Rescuer clinicians tend to put others’ needs before their own, struggle to set boundaries and take on too much, which can ultimately lead to exhaustion and burnout. It may even unintentionally harm those they aim to help. For more on this, see our article Personality traits contributing to stress. |
| Cognitive overload | Cognitive overload – the strain on working memory during tasks – is linked to higher risk of burnout. This depends on the difficulty of the task, our level of skill and the mental effort required to access and process information. Reducing this load, such as by using AI tools, may support wellbeing. |
| Society of Occupational Medicine, 2023, JAMIA Open 2023; 6:ooad079 | |
Specific causes of burnout in dentists
In dentists, increased rates of stress and burnout are associated with (Healthcare 2024; 12:2366df, GDC, 2021):
- Being less experienced.
- Working as a general practice dentist.
- High levels of NHS work (rather than private practice).
- Long working hours or working on weekends/overnight.
- Low job satisfaction.
- Having a high number of patients or working under constant time pressure.
- Isolated working patterns and lack of support from colleagues.
The impact of burnout
Burnout has serious consequences for both clinicians and patients.
A BMJ systematic review found that physicians across multiple specialities who experience burnout show changes that affect many aspects of professional practice (BMJ 2022;378:e070442):
- Patient safety: burnout was linked to more safety incidents, including medication errors and diagnostic delays, with emotional exhaustion being a major contributing factor.
- Professional behaviour: burnout was associated with low professionalism, including suboptimal patient care, failure to follow clinical guidelines and poorer communication. In particular, depersonalisation undermined professional behaviour and patient experience.
- Patient satisfaction: burnout was associated with lower patient satisfaction, reflecting the combined effects of safety incidents and reduced professionalism.
- Career impact: clinicians with burnout were more likely to feel dissatisfied with their jobs, regret their career choice, consider leaving medicine and report lower productivity or lack of career development.
A similar negative pattern has been shown in dentists. A systematic review of dental professionals found that burnout was associated with (Healthcare 2024;12:2366):
- Lower quality of care, including increased patient safety risks from errors of judgement, misdiagnoses and technical mistakes.
- Poor sleep, fatigue, anxiety, stress and increased alcohol consumption.
- Higher risk of job dissatisfaction, workplace change or leaving the profession.
- Greatest vulnerability among younger dentists and those in high-intensity surgical specialties.
Spotting burnout in ourselves and our colleagues
Burnout often develops gradually, and can present differently in each person, making it easy to miss – especially in teams that are busy and under pressure. Colleagues are often good at spotting these early signs so it’s important to stay attuned, offer support and raise concerns when needed. Remote staff and new team members may need extra connection and check-ins because signs can be harder to spot. We discuss some skills for starting a conversation about wellbeing with a colleague in our article, Starting mental health conversations.
Common signs of burnout include (Society of Occupational Medicine, 2023):
| Emotions |
|
| Thoughts and cognitions |
|
| Behaviour |
|
| Physical symptoms |
|
| Social interactions |
|
Stages of burnout
In his book, Burnout-free working (JKP, 2025), Richard Duggins outlines three stages of burnout:
The plateau: coping on empty
This stage can last months or even years. People keep functioning under pressure, appearing competent while feeling increasingly drained. They begin to let go of restorative activities – such as seeing friends, exercising or resting – and focus all their energy on meeting demands at work and home. Isolation grows, but shame and fear of judgment often prevent them from asking for help. Thinking narrows into self-critical beliefs: I have to keep going, I can’t let anyone down or If I stop, I’ll be seen as weak. Despite emotional numbness, irritability and poor sleep, we keep pushing on, coping on empty and edging closer to burnout.
The burnout cliff: sudden collapse
The burnout cliff often comes as a shock – to the person themselves and those around them. Many say they didn’t see it coming because they had been ‘coping’ by cutting out anything non-essential and ignoring their own warning signs. Then, a seemingly minor demand tips everything over the edge. Suddenly, they’re no longer able to function at work. Their mood crashes, physical symptoms emerge and urgent time off or a major reduction in responsibilities becomes unavoidable.
What makes this moment so distressing is not just the collapse, but the loss of a role that has become central to their identity. Feelings of shame, fear and failure are common, alongside self-critical thoughts such as I should have tried harder or I’ve let everyone down. But this isn’t a sudden event – it’s the final stage of a long, hidden decline, driven by a culture that equates strength with silence and prioritises productivity over wellbeing.
Recovery: rebalancing and renewal
Recovery begins by making space to rest and reflect. It often brings the realisation of just how long someone has been running on empty and what they’ve sacrificed to keep going.
Small, restorative steps – such as reconnecting with others, spending time outside or simply pausing – help rebuild energy. As these become more regular, unhelpful beliefs about productivity and self-worth can start to shift.
Recovery isn’t about going back to how things were. It’s about finding a more sustainable way forward, with clearer boundaries, greater self-awareness and a kinder inner dialogue: I coped the only way I could. Now I’m choosing differently.
What can we do to tackle burnout?
Burnout has multiple complex causes so there is no single solution. Addressing it requires more than simply promoting ‘resilience’ in individual clinicians; it also requires systemic change and improved working conditions that enable staff to thrive. The most effective approach is likely to combine strategies at multiple levels, tailored to the needs of individuals and organisations. These include:
- Primary interventions: changes to the workplace that can help prevent burnout. This is essential because once clinicians have reached the exhaustion phase, it can take a significant time to recover.
- Secondary interventions: supportive strategies that help individuals and teams cope better with work-related stress and reduce the risk of burnout.
- Tertiary interventions: clinical treatment and workplace adaptations for individuals already experiencing burnout, with a focus on recovery, rehabilitation and a sustainable return to work.
In the next part of the article, we look at each of these in more detail.
Primary prevention of burnout
Preventing burnout is essential – not only for individual wellbeing, but for the long-term sustainability of the healthcare workforce. In high-pressure environments such as primary care and dentistry, the steady accumulation of relentless demand, emotional strain and moral distress may go unnoticed until it begins to cause real harm.
Primary prevention involves taking proactive steps to create healthier working environments that support psychological safety, reduce systemic pressures and promote everyday wellbeing. The goal is to make burnout less likely in the first place by embedding support into the way teams and systems operate. This includes:
|
Sustainable workload and better support
|
|
| Supportive workplace culture |
|
| Effective management and leadership |
|
| Encourage autonomy and meaningful work |
|
| Monitor wellbeing at work |
|
| Support clinicians with diverse needs |
|
| NEJM 2024;391:1519, Society of Occupational Medicine, 2023, JAMIA Open 2023; 6: ooad079, CIPD, 2024: Supporting mental health at work | |
This is an important reminder that burnout prevention isn’t about urging individuals to be tougher, push through or simply cope better. It’s about creating the conditions where people are able to do their jobs effectively and sustain their wellbeing. Real prevention focuses on the system around the work – not just the resilience of the people doing it.
Secondary prevention: improving support for individuals and teams
Secondary prevention focuses on recognising and responding to early signs of burnout before they escalate into more serious or lasting difficulties. While primary prevention aims to reduce systemic pressures and minimise risk, secondary prevention involves taking timely action when stress begins to take a visible toll. This means noticing subtle changes in behaviour, mood or performance, and offering support early.
Acknowledging these early warning signs creates a valuable opportunity to reverse the trajectory and prevent burnout from becoming entrenched. This involves practical strategies to identify and address early signs in ways that support wellbeing and maintain functioning – both for individuals and teams. These include:
| Individual interventions |
Individual interventions can improve emotional exhaustion, stress, anxiety, depression, resilience and quality of life. However, the strength of the evidence remains limited. Strategies may include:
|
| Team support |
Many primary prevention measures, such as managing workload and ensuring adequate staffing, also help limit rising stress in teams. In addition, strategies to support and strengthen teams can be protective against burnout, helping clinicians cope with the emotional demands of care and creating a culture where wellbeing is valued. Practical steps include:
|
| NEJM 2024;391:1519, Society of Occupational Medicine, 2023, JAMIA Open 2023; 6: ooad079, CIPD, 2024: Supporting mental health at work, BMJ Open 2023;13:e071203, BMC Health Services Research 2025;25:731 | |
The fast pace and constant demands of primary care can make it difficult to notice or respond to early signs of burnout. Conversations about wellbeing may get squeezed out, even with the best intentions. That’s why it’s essential to prioritise efforts to build a culture that supports early recognition. This takes time and care – but it’s a vital part of sustaining healthy, effective teams over the long term.
Recovery and rehabilitation after burnout
Tertiary strategies focus on supporting recovery for those already experiencing burnout, and, where possible, enabling a sustainable return to work. At this stage, the emphasis shifts from prevention to active treatment and rehabilitation. Recovery often requires coordinated support between individuals, teams and organisations, with an approach that is compassionate, flexible and responsive to the complexity of each situation.
Recovery from burnout is rarely quick or straightforward, and the process can include setbacks. It may involve periods away from clinical duties, psychological therapy and adjustments to workload, expectations or responsibilities. It typically requires attention to multiple contributing factors – both personal and systemic. Support should be tailored to the individual, recognising the stage and severity of burnout, and be delivered in a way that promotes long-term wellbeing and successful reintegration into work.
Burnout is not just a personal issue – it usually reflects wider systemic and organisational pressures. Recovery therefore demands more than individual coping; it calls for organisational commitment to shared responsibility, supportive leadership and access to occupational and mental health services.
The evidence on effective treatment for burnout remains mixed. While many interventions show short-term benefits, they often have limited impact on longer-term outcomes such as sustained wellbeing or return to work. There’s a need for better-designed studies with long-term follow-up; a stronger focus on organisational change; and consistent definitions and measures of burnout across research (Burnout Research 2017; 4:1, Society of Occupational Medicine, 2023).
Some key steps in burnout treatment and recovery include:
| Early identification and awareness |
|
| Rest and time off work |
|
| Seek professional support |
|
| Talking therapies |
|
| Physical or behavioural |
|
| Combined approaches organisational change |
|
| Burnout Research 2017; 4:1, Society of Occupational Medicine, 2023 | |
How to plan and support the return to work
Planning a return to work is a key part of the recovery process – not a final step. It should begin with early, collaborative discussions to establish a phased, realistic approach that is tailored to the individual’s needs. Involving the individual, their line manager and occupational health in this process helps ensure that support is person-centred and recovery-focused.
| Planning an effective return to work |
|
| Monitoring after return |
|
Putting these strategies into practice can be challenging in busy healthcare settings. But small actions – such as really listening, offering flexible adjustments and showing a genuine commitment to improving wellbeing – can make a huge difference. The quality of support during a return to work is also crucial: the more responsive and tailored it is, the greater the chance of a successful and sustained recovery. We cannot expect people to return to the same conditions that contributed to burnout. Meaningful recovery requires lasting changes that make wellbeing a core part of everyday working life.
Personal microskills for preventing burnout
We cover this in more detail in our articles Building resilience and Roadmap to wellbeing: microskills for positive change, but here are a few quick tips:
| Find out what refuels you |
Notice what you stop doing when you feel stressed or busy – this is often something that may re-energise or refuel you. Book it in now! This might be seeing friends, going swimming or getting outside. You can also try the five ways to wellbeing:
|
| Prioritise and say ‘no’ when needed | We all know that we need to prioritise and say no more often – but knowing what to say no to can be hard. With limited time each day, it’s essential to take control of how we spend it and be intentional about what we commit to. If something feels just a bit too much, pause and ask yourself: Do I really want to do this? Do I have time? Is this a current priority? Will I enjoy it? If the answer to any of these is no, it’s OK to say no – so you can say a fuller yes to what matters most. See our article Communicating our needs and setting boundaries for more on this. |
| Focus on what you can control |
Working as a health professional brings huge pressures, many of which are beyond our control. Focusing on these pressures can increase stress and make us feel powerless, while distracting us from what we can influence: our actions, responses and daily choices. These may not always be easy, but we often have more agency than we realise. When feeling overwhelmed, it’s hard to see our options clearly. Take a moment to pause and imagine your ideal life, job or health. If this looks very different from your current reality, ask what small changes are within your control. Could you reshape your role, adjust your routine or take one step toward a goal? Even small shifts can restore a sense of control and energy. |
| Leave work at work |
Many of us are striving for that elusive work–life balance, and feel that if we only spent longer at home, we’d find it. But it’s often less about how much time we spend away from work and more about the quality of that time. Creating a clear boundary between work and home helps. One effective way to do this is to build in a ‘decompression zone’ – a short period after work to reset. This could be part of your commute, a walk, a jog, a shower or even a few minutes of quiet reflection. The key is to consciously transition between work mode and home life. You can also take control by setting clear boundaries around checking emails or results outside of work hours. Something as simple as switching off your phone or leaving it in another room can make a real difference in helping you leave work at work. |
A final thought…
Although this article may make for sobering reading, it reflects the reality that many clinicians face every day. The encouraging news is that the wellbeing of healthcare professionals is increasingly being recognised as fundamental to delivering safe, high-quality care.
Support is available, yet many clinicians continue to delay seeking help. They minimise their own needs or push on long after things have become unsustainable. If you're finding things difficult, prioritise your own wellbeing and reach out for support – not as a last resort, but as a vital act of care for yourself. Practising self-care and compassion isn’t a luxury. It’s what helps you sustain your energy, keep perspective and continue engaging in work that matters, while still having the capacity to enjoy other parts of your life.
|
Burnout in health professionals
|
|
|
Useful resources: Websites (all resources are hyperlinked for ease of use in Red Whale Knowledge)
Podcasts
Books
|
This information is for use by clinicians for individual educational purposes, and should be used only within the context of the scope of your personal practice. It should not be shared or used for commercial purposes. If you wish to use our content for group or commercial purposes, you must contact us at sales@red-whale.co.uk to discuss licensing, otherwise you may be infringing our intellectual property rights.
Although we make reasonable efforts to update and check the information in our content is accurate at the date of publication or presentation, we make no representations, warranties or guarantees, whether express or implied, that the information in our products is accurate, complete or up to date.
This content is, of necessity, of a brief and general nature, and this should not replace your own good clinical judgment or be regarded as a substitute for taking professional advice in appropriate circumstances. In particular, check drug doses, side effects and interactions with the British National Formulary. Save insofar as any such liability cannot be excluded at law, we do not accept any liability for loss of any type caused by reliance on the information in these pages.
Here is the link to our terms of use.