 Cancer and frailty
Cancer and frailty
-
1. Cancer and frailty
- 1.1 What is frailty and why does it matter in cancer?
- 1.2 Frailty assessment: who, when and how?
- 1.3 Frailty screening at point of referral
- 1.4 Using frailty assessments in cancer care
- 1.5 Prehabilitation: an opportunity to improve outcomes for our frail patients
- 1.6 Cancer care in moderate–severe frailty
This Pearl is provided as free content. Here is the link to our terms of use
Cancer and frailty
Cancer and frailty
Frailty is common in people with cancer, and those who are frail have worse quality of life and reduced cancer survival. Frailty leads to higher risk of treatment toxicity and increased surgical complications (Joint Collegiate Council for Oncology 2023).
More than a third of cancer diagnoses, and over half of cancer-related deaths, are in people aged 75y or older. Older adults are more likely to be frail and have co-existing disability and comorbidities, but frailty can be present at any age.
Failure to consider frailty in cancer-related decision-making risks harm from over-investigation and overtreatment.
This article was last updated in November 2025.
You may find our related articles useful.
- Frailty.
- Advance care and end-of-life planning in multimorbidity and frailty.
- Frailty annual review: the comprehensive geriatric assessment.
- Lifestyle medicine for patients after a diagnosis of cancer.
- Polypharmacy, medication reviews and deprescribing.
What is frailty and why does it matter in cancer?
Frailty is characterised by a loss of physiological reserve to cope with even minor external stressors. It develops due to age or illness-related degeneration of multiple physiological systems. Stressors might include a diagnosis of, and treatments for, cancer (Clin Interv Aging 2023;18:505).
Cancer and its treatment will impact on the reserve of any patient, however medically fit they are. In the severely frail, there is likely to be reduced benefit of treatment and a high chance of worsening frailty. Frail patients are at increased risk of postoperative complications, chemotherapy intolerance, disease progression and death (CA Cancer J Clin 2017;67:362).
Frailty assessment informs decisions about treatment. It is commonly performed in secondary care, often by the multidisciplinary team. There is also increasing interest in the importance of re-evaluating frailty during treatment to inform ongoing management (Clin Interv Aging 2023;18:505).
Frailty assessment: who, when and how?
Who should be assessed for frailty?
Everyone referred with suspected cancer, particularly those aged ≥65y, should be assessed for frailty (Joint Collegiate Council for Oncology 2023).
When should we do a frailty assessment?
A frailty assessment should be done at every step along the cancer journey in order to inform treatment decisions and ongoing care (Joint Collegiate Council for Oncology 2023).

Who should do the assessment?
The NHS RightCare Toolkit advocates that all healthcare staff can recognise and record frailty.
Which frailty assessment tool should we use?
All suspected cancer pathway referral forms will include a frailty assessment, although different scales may be in used in different areas. What assessment tool is used in your area?
Frailty assessment tools, even in their simplest form, have been demonstrated to be more relevant than performance status scales such as the WHO performance status (Joint Collegiate Council for Oncology 2023).
The Rockwood Clinical Frailty Scale was developed from the Rockwood Frailty Index (Tech Innov Patient Support Radiat Oncol 2020). It matches patients against 9 descriptions of increasing levels of frailty using words and pictures, allowing rapid assessment without the need for clinical expertise. Although only formally validated for people ≥65y, there is good evidence to support its use as a screening tool in younger people being referred for suspected cancer (Joint Collegiate Council for Oncology 2023).
Frailty tools are also embedded in electronic health records, automatically generating a frailty score from any coded input.
Have you ever noticed or used the incorporated frailty assessment tool in your clinical system?
Frailty screening at point of referral
In its guidance on suspected cancer, NICE advises clinicians to consider “the individual needs, preferences and values of their patients or the people using their service” (NICE 2015 (updated 2025), NG12).
Before making a suspected cancer pathway referral, we should:
- Ask about our patients' preferences for being involved in decision-making about referral options and further investigation.
- Make sure that the patient or their advocate is aware that they are being referred to a cancer service.
- Advise what to expect from the referral: investigation and possible treatments.
- Discuss the risks, benefits and consequences of referral in the context of each person's life and what matters to them (NICE 2021, NG197).
Why is accurate referral information so important?
Assessing frailty enables us to (Joint Collegiate Council for Oncology 2023):
- Assess the appropriateness of fast-track referral:
- We can gauge the risks and benefits of diagnostic investigations and cancer treatments, allowing informed shared decision-making with patients.
- Provide accurate information to the specialist team as part of the referral process:
- Secondary care triage of suspected cancer pathway referrals will result in some patients having invasive investigation without further clinical assessment in secondary care. This may not be safe or appropriate for all.
- Assess baseline frailty scores:
- Some patients may present acutely unwell, and appear more frail at diagnosis than is their true baseline, risking missed opportunities for referral and active treatment (Clin Interv Aging 2023;18:505).
- Allow optimisation of frailty-related issues, improving quality of life and tolerance of cancer treatments.
What information should I include in a suspected cancer referral?
The Red Whale Cancer team shares below some pearls of wisdom on important comorbidities to consider when making a suspected cancer referral. By ensuring we share this information with secondary care, we can reduce the risk of unnecessary or harmful investigations.
Comorbidities to consider include:
- Those at risk of acute kidney injury (CKD, diabetes, medications such as diuretics or digoxin):
- Care needed with bowel preparation for colonoscopy and contrast CT because these can cause significant fluid depletion.
- Heart failure/cardiac arrhythmia:
- Bowel preparation may cause electrolyte disturbance, worsening heart failure or triggering an arrhythmia.
- Severe mobility issues (e.g. movement disorders, obesity, musculoskeletal conditions):
- May need additional time for appointments, adapted equipment and facilities, or modified positioning.
- Mental capacity/memory impairment (e.g. learning disability, cognitive impairment):
- May need support to carry out pre-appointment preparation.
- Consent may be more complex or require best-interest decision-making.
- Sedation may be needed for some investigations.
- Mental health (e.g. severe mental illness, depression/anxiety):
- Difficulty engaging with secondary care investigations.
- Worsening of mental illness related to cancer diagnosis or treatment.
It is helpful to highlight these comorbidities on the referral form and discuss any concerns with the patient or their carer. We should involve specialist teams early and ask advice and guidance about appropriate referral routes if we are unsure. Of course, this list is not exhaustive and we should make an individual assessment of risks for each patient.
Is fast-track referral appropriate?
Deciding that someone may have cancer but that fast-track referral may not be in their best interests can be a difficult clinical dilemma. Communicating this to the patient and their family can also be challenging.
Some tips and suggestions:
- If you feel unable to make an informed decision about this with a patient or their advocate, explain your concerns, and suggest that to ensure the best route of investigation, you wish to discuss this with colleagues/specialists. Arrange timely follow-up.
- If referral made by any route has the aim of only confirming diagnosis for a patient (where active treatment is unlikely to be appropriate or is not wanted), make this clear on the referral.
Using frailty assessments in cancer care
Frailty assessments allow care teams to tailor management to the patient.
What might this look like?
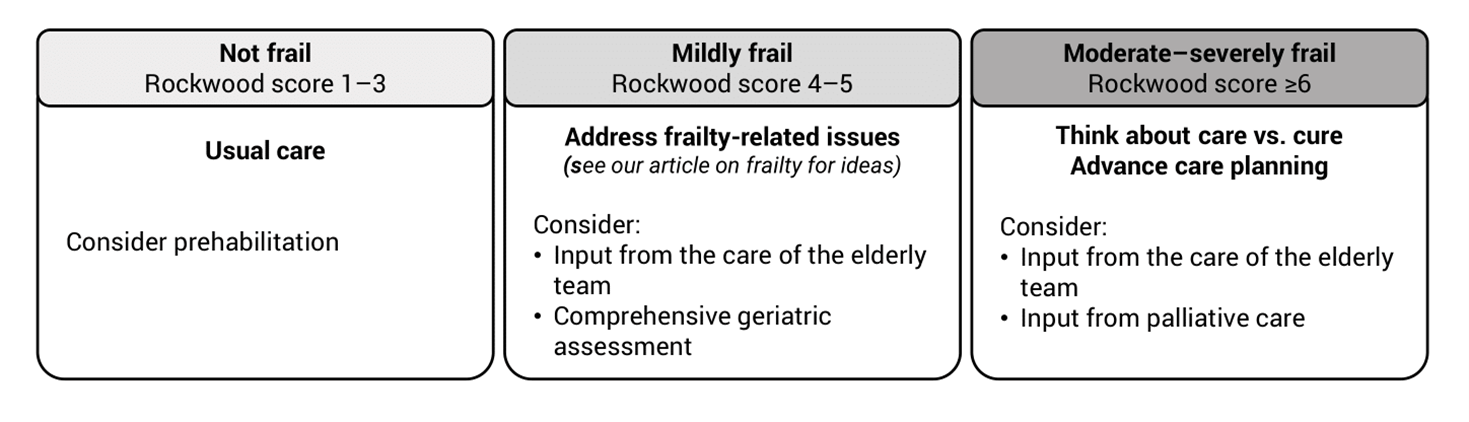
Prehabilitation: an opportunity to improve outcomes for our frail patients
Frailty assessment is not meant to exclude all patients with preidentified frailty from cancer therapy, but to make treatment in these patients as safe as possible through additional supportive measures (Clin Interv Aging 2023;18:505). Spotting frailty at the time of referral is a great opportunity to consider prehabilitation, optimising the outcomes for our patients (Prehabilitation resources for healthcare professionals | Macmillan Cancer Support).
Comprehensive geriatric assessment, followed by interventions to improve frailty deficits, has been shown to improve treatment tolerance, particularly in elderly patients receiving systemic cancer therapy, with a low NNT of 5–10 (Clin Interv Aging 2023;18:505).
We have included much more detail on how to achieve this in our articles Frailty annual review: the comprehensive geriatric assessment and Lifestyle medicine for patients after a diagnosis of cancer, but here are some key suggestions.
Medication review and managing comorbidities
- Consider a medication review, particularly for those on multiple medications. Addressing polypharmacy through deprescribing of unnecessary medications can reduce tablet burden and the risks of drug interactions and electrolyte disturbance from bowel preparation (if needed) (The Lancet Oncology 2015;16:e333). Have you heard of the STOPPFrail toolkit? See our article Polypharmacy, medication reviews and deprescribing for more information.
- Optimise management of comorbidities such as COPD, heart failure and diabetes. Seek advice and guidance or support from colleagues if needed.
Lifestyle and modifying risk factors
- There is evidence that smoking cessation and reduction of alcohol and other harmful substances improves prognosis in breast cancer (JAMA 2023;6:e2311673), lung cancer (JTO 2022;17:623) and upper GI cancer (J Clin Oncol 2018;36:83)
- Regular physical activity has been shown to improve prognosis in a range of cancers (Med. & Science in Sports and Exercise 2019;51:2375).
- Lifestyle improvement facilitates management of comorbidities.
Nutrition and sarcopenia
Optimising nutritional status while awaiting investigation can improve tolerability of investigations and treatments.
- Regularly evaluate nutritional intake, weight and BMI, starting at referral and repeating throughout the cancer journey as needed (ESPEN, guidelines on nutrition in cancer patients (Clin Nutr 2021;40:2898).
- Consider whether a MUST score and/or dietitian referral are needed.
- Offer information on optimal diet (see link in useful resources for Macmillan patient booklet).
- Short-term prescription of nutritional supplements for those affected by dysphagia or anorexia symptoms may be appropriate, dependent on local formularies and guidance (ESPEN, guidelines on nutrition in cancer patients (Clin Nutr 2021;40:2898).
Sarcopenia is the loss of muscle mass often associated with chronic disease and ageing. It can lead to mobility issues, including difficulty rising from a chair, slower walking and general weakness, and has been associated with increased risk of treatment toxicity and worse long-term outcomes in cancer patients (Transl Cancer Res 2020;9:5760).
- Sarcopenia can be masked by obesity – so-called sarcopenic obesity.
- Offer advice on gentle aerobic and resistance exercise, and on nutrition, including increased protein intake.
Psychological support
- A potential or confirmed diagnosis of cancer will inevitably have some psychological impact.
- We should remain alert for a response beyond a normal adjustment reaction (BMJ 2018;361:k1415). This can influence willingness to accept and ability to tolerate ongoing treatments. See our article on Cancer and mental health for more on this subject.
Cancer care in moderate–severe frailty
What if continuation of treatment may be inappropriate due to extreme frailty?
Should discontinuation of cancer treatment be considered?
This can be emotive and challenging. Remember, though, that a patient is sometimes waiting for a clinician to recognise and suggest that treatment is becoming too much of a burden. They may be relieved that you are giving them an opportunity to question reasons for continuation of treatment. Our role here is not to make a decision about treatment, but to enable an open and honest discussion. It may also be appropriate to liaise with the specialist team.
- Involve the appropriate people in discussions and make use of the multidisciplinary team as needed in ongoing management. This may include community frailty teams, care home staff and specialist palliative care teams.
- Communication skills and advance care planning are key. See our articles Advance care planning, including resuscitation decisions and Advance care and end-of-life planning in multimorbidity and frailty for more on this.
|
Cancer and frailty
|
|
|
Useful resources: Websites (all resources are hyperlinked for ease of use in Red Whale Knowledge) |
This information is for use by clinicians for individual educational purposes, and should be used only within the context of the scope of your personal practice. It should not be shared or used for commercial purposes. If you wish to use our content for group or commercial purposes, you must contact us at sales@red-whale.co.uk to discuss licensing, otherwise you may be infringing our intellectual property rights.
Although we make reasonable efforts to update and check the information in our content is accurate at the date of publication or presentation, we make no representations, warranties or guarantees, whether express or implied, that the information in our products is accurate, complete or up to date.
This content is, of necessity, of a brief and general nature, and this should not replace your own good clinical judgment or be regarded as a substitute for taking professional advice in appropriate circumstances. In particular, check drug doses, side effects and interactions with the British National Formulary. Save insofar as any such liability cannot be excluded at law, we do not accept any liability for loss of any type caused by reliance on the information in these pages.
Here is the link to our terms of use.