
This Pearl is provided as free content. Here is the link to our terms of use
Grief
Grief
“I don’t think you ever get over it, but I am beginning to see that there might be a life out there for me, without John. It’s a very different life from what we imagined together…but there are some things I am starting to feel excited about…”. This was said to me many years ago by a woman whose husband had died about 6 months previously, shortly after he had retired.
This article was reviewed in December 2025.
We would like to thank Dr Lucy Selman, Professor of Palliative and End-of-Life Care at the University of Bristol, for her expert feedback on this article.
Understanding grief and loss
Loss is an inevitable part of life, and grief is a natural response. It is not an illness or a mental health disorder, but a normal psychological process. Even so, coping with a significant loss can be among the most challenging experiences a person faces.
Grief will often follow a significant bereavement such as the death of a family member, close friend or colleague. It can also arise after a non-death loss – the real or perceived loss of something meaningful. These losses can be sudden or gradual, public or private, temporary or permanent, but all involve recognising that something is no longer as it once was. Examples include loss of a job, breakdown of a relationship, a significant change or loss of physical ability, loss of cultural identity when migrating to a new country, or realising that a hoped-for future is no longer possible (Adultspan Journal 2020;19:118).
Health professionals are also vulnerable to grief. Many clinicians encounter repeated experiences of death and dying in their work, which can carry significant emotional, psychological and physical effects. These reactions are often hidden or managed privately because patient care and workplace demands tend to take priority. Personal bereavements and other experiences of loss can also affect how clinicians respond to patients presenting with grief. They may strengthen empathy, rapport and coping skills, but can also heighten vulnerability, with past losses resurfacing when caring for certain patients (Health Serv Insights 2025;18:11786329251344772). We discuss ways to support clinicians experiencing grief in more detail below.
Early grief responses
Grief is unique to each person, and an individual may experience bereavements very differently at different points in their life. Culture, ethnicity and spiritual beliefs may also influence how grief is expressed and how people cope.
In the early period after a loss, grief often feels overwhelming and can disrupt daily life. People may be surprised by the intensity of their emotions or their difficulty focusing on everyday tasks, or by experiencing brief sensory perceptions of the deceased.
Common early grief responses can include a wide variety of symptoms:
| Emotions |
|
| Thoughts and cognitions |
|
| Behaviours |
|
| Physical reactions |
|
| (BMJ 2017;357:j2016, BMJ 2017;358:j2854; Lancet 2007;370:1960) | |
For most people, grief gradually lessens over time as they adapt to life after loss. Many find new ways of living with the absence, drawing on personal coping strategies, social support and cultural or spiritual resources. However, a minority continue to experience enduring distress that can interfere with daily life. Several models have been developed to describe the process of grief and how adaptation unfolds.
The grief process
Grief does not follow a straight path, and there is no single way that people adapt after loss. Various models have been developed to help make sense of these experiences. They are not rigid formulas, but flexible frameworks that describe the diverse emotional, cognitive and behavioural responses that may arise.
Stages of grief
The well-known ‘five-stages’ model of grief (Kubler-Ross, 1969) describes it as proceeding along a series of predictable stages. This can be useful for understanding some of the different reactions people may have to a significant loss.

Kubler-Ross acknowledged that people may not move through these stages in a fixed order, and that some individuals may stay longer in one stage or move back and forth between them. However, the model has been criticised for presenting grief as a series of predictable steps. In practice, grief is highly individual: people may experience a range of different emotions that may appear in any order, recur over time or fall outside the five stages altogether. Individual and cultural differences can both influence how these processes unfold (Lancet 2007;370:1960).
The dual-process model
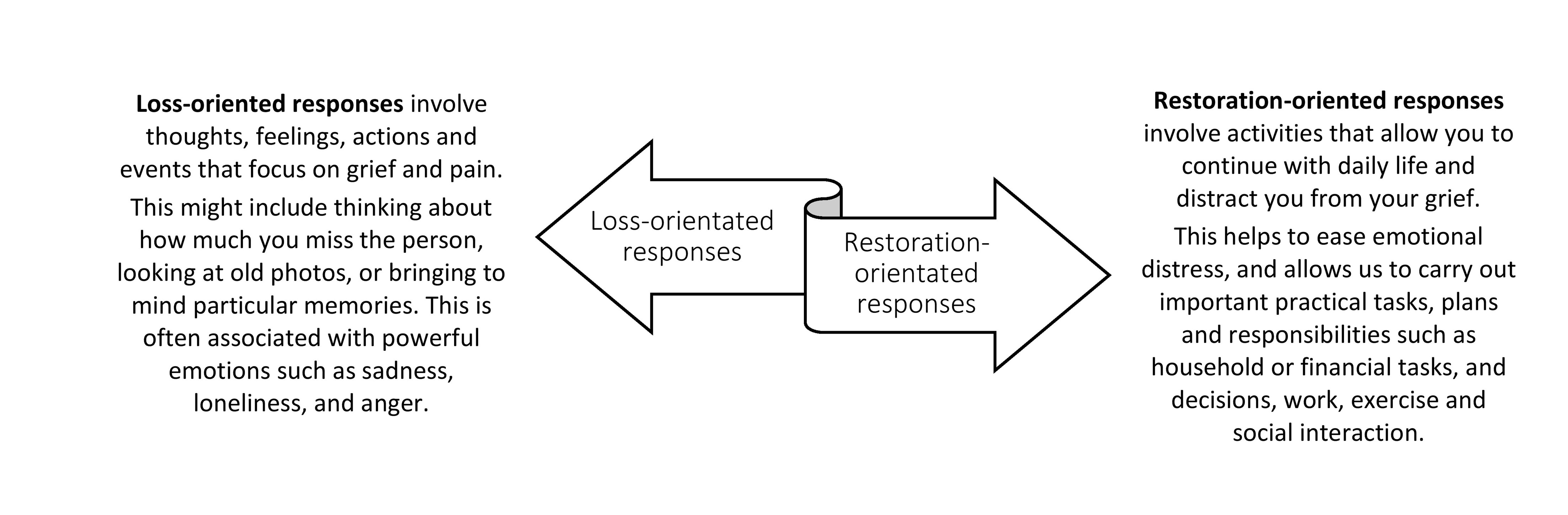
The dual-process model (Stroebe and Schut, 1999) suggests that grieving involves moving back and forth between two modes of coping:
- Loss-oriented coping: directly confronting and experiencing the pain of the loss.
- Restoration-oriented coping: attending to the practical and social changes that follow bereavement.
This oscillation between loss and restoration is considered a normal, adaptive part of the grieving process, allowing people to face their loss in manageable steps while continuing with daily life.
The task-based model
The TEAR model describes four ‘tasks’ of healthy grief (Worden, 2008). There is no recommended or specific order in which to achieve these. Instead, it highlights the active steps many people take as they gradually adapt to bereavement:

- To accept the reality of the loss: moving from shock or disbelief towards acceptance is the first step in adapting and moving forward. Rituals such as funerals and memorial services can help with this.
- Experience and process the pain of loss: this involves facilitating the safe expression of all the natural grief reactions.
- Adjust to a world without the deceased: we slowly adapt to the change in our life, and start to see the possibility of purpose, meaning and happiness.
- Re-invest in a new reality and a new life: finding ways to move forwards through life, while finding meaningful ways to keep a connection to the person who died.
Supporting people with grief
- For many bereaved people, support from family, friends and community networks is enough to help them adjust to the painful reality of loss, without the need for formal intervention.
- Others may also benefit from bereavement support from a range of statutory, community, charitable and voluntary organisations, including the primary care team, bereavement counsellors, social care workers and hospice and palliative care services. We have included some resources in the links below.
The role of primary care
- Although bereavement care is recognised as part of primary care, many clinicians report feeling unsure or insufficiently prepared to support people experiencing grief, even after training. There may be concerns about managing time and workload pressures, plus health professionals supporting distressed, grieving patients can suffer a personal emotional toll. We may also fear medicalising grief or intruding into a private life event, particularly if we do not know the individual or their family well.
- There may also be uncertainty and a lack of awareness among clinicians about how and when to recognise complicated grief or prolonged grief disorder, or what to do in response.
- Nevertheless, primary care clinicians are highly-skilled communicators who are well placed to support patients with their experiences of grief, based on a strong, trusting relationship with the patient.
- Following a bereavement, many patients value receiving acknowledgement and contact from their GP, and the opportunity to speak about their grief in primary care. However, practical and administrative challenges may make this difficult, particularly if a deceased person was registered at a different practice from the bereaved patient.
(BMJ 2017;358:j2854; BJGP Open 2021;5:BJGPO.2021.0008).
Very brief advice framework for supporting people who are grieving
The RCGP’s A Compassionate Bereavement Response provides a simple structure for offering brief, effective support in primary care for those who are grieving. It has four steps:
| Brief advice | What we might say |
| ACKNOWLEDGE the loss | [Use person’s name], I am so sorry to hear... |
| ASK about current support |
How are you getting on? Who else close to you has been affected by the loss? Who do you have around you for support? |
| ADVISE on suppport options |
Support can make a real difference for many people. What other support do you think might help you right now?. Some find it through friends, family or their community, and there are also organisations that can help. Is there anyone you feel able to reach out to? You can come back and see me at any time if you need more support. |
| ACT on the person’s response and record the bereavement |
Show kindness and give space for their response. Offer information about local and national support organisations. Seek guidance from a senior colleague if you have any concerns. |
Primary care microskills for grief
- Offer bereaved patients the opportunity to talk about the person who has died, their grief and how they have been coping.
- When relevant, openly discuss patient questions or concerns about medical care received by the person who died, or about the last days of life.
- Encourage social connection and support, a healthy lifestyle, and provide advice on sleep hygiene.
- Over time, the patient will benefit from reducing avoidance of reminders of the loss, and slowly beginning to create a new life. Use brief behavioural activation to encourage engagement with valued activities such as family life, work, hobbies, physical activity and self-care activities.
Prolonged grief disorder
Prolonged grief disorder is now recognised as a mental health condition in both ICD-11 (ICD-11, 2022) and DSM-V (APA, 2022). Both define it as a persistent and disabling grief response that extends beyond expected cultural and social norms of grieving. They differ slightly in how long symptoms must persist before a diagnosis can be made, but share substantial overlap in emphasising separation distress, emotional pain and functional impairment as core features.
Around 3–10% of people bereaved by natural causes develop prolonged grief disorder, with higher rates after sudden or traumatic losses (NEJM 2024;391:1227). However, prevalence remains uncertain due to inconsistent diagnostic criteria and wide variation by circumstances of death.
Risk factors for prolonged grief disorder include (NEJM 2024;391:1227):
- Pre-existing depression or significant symptoms of grief before the loss.
- Previous traumatic stress or earlier traumatic loss.
- Violent or sudden deaths such as suicide, accident, unexpected medical illness, natural disaster or war.
- Use of alcohol or other substances.
- Family conflict, social isolation or lack of support.
- Experiences of poor care or lack of comfort, or insensitive communication from the healthcare team.
| Key features of prolonged grief disorder |
|
Useful questions to assess for prolonged grief disorder
- Can you tell me about the person who died and your relationship with them?
- How has life been for you since the loss?
- In what ways is your grief affecting your daily life?
- Are there things you avoid, or feel preoccupied with, because of the loss?
- What helps you cope, and who do you feel able to turn to for support?
- Do you feel able to imagine a future, or does that feel very difficult right now?
(BMJ 2017;357:j2016, Clin Psychol Rev 2024;107:102375, NEJM 2024;391:1227, Lancet 2025;405:1621)
Are we just medicalising grief?
- Grief is not an illness – it is a natural response that occurs as a bereaved person adapts to their loss. There is a concern that labelling prolonged grief disorder as a mental health condition could stigmatise this group, or undermine individual coping skills or seeking support from friends and family.
- However, giving a diagnosis of prolonged grief disorder may be helpful for many individuals. It can be a comfort and a relief to the bereaved person to help them understand their experiences, and shift from self-blame about ‘being unable to cope’ into confidence that treatment might help (BMJ 2017;357:j2016).
Can prolonged grief disorder be prevented?
Evidence for prevention remains limited. Universal approaches for people without risk factors may have little benefit, whereas targeted support for higher-risk groups shows more promise, with small to modest effects. Family-focused therapy in advanced cancer care, begun during palliative care and continuing into bereavement, has been shown to reduce risk compared with standard care. Cognitive behavioural interventions may also help, as can family-based support in settings such as cancer or intensive care.
Some coping patterns after bereavement may increase the risk of prolonged grief disorder. Persistent avoidance of reminders, repetitive rumination about the loss or its unfairness, and ongoing attempts to maintain closeness with the deceased may all predict later difficulties if continued beyond the early months. While maintaining a bond can be a healthy part of grieving, it becomes problematic when it prevents adaptation and engagement with ongoing life.
In primary care, we can support healthy grieving by listening, encouraging social interaction and promoting gentle re-engagement with daily life – while helping patients recognise when avoidance or rumination may increase the risk of grief becoming persistent and disabling. We can also signpost to the many support services available – see below for some links.
(Psychiatry Res 2024;339:116060, Lancet 2025;405:1621, BMJ 2017;357:j2016)
Treating prolonged grief disorder
A tiered approach to bereavement care can be useful. While most people adapt with support from family, friends or community services, a smaller group may need specialist psychological intervention. Access to such care, however, remains uneven and limited in many areas.
-
Psychological therapy is the first-line approach: the goal is to support acceptance of the loss, and re-engagement in a meaningful life without the deceased. CBT has the strongest evidence base, reducing distress and aiding adaptation by addressing memories, beliefs and unhelpful coping behaviours. Key components of therapy include:
- Behavioural activation: restoring valued roles and activities, while reducing avoidance and rumination.
- Cognitive techniques: challenging negative beliefs about the self, the future or the safety and predictability of the world, particularly after violent loss.
- Exposure: reducing avoidance by revisiting memories, situations or objects linked to the loss.
- Specialised CBT and family-based programmes tailored for children and young people have also shown effectiveness across cultural contexts.
- Approaches such as eye movement desensitisation and reprocessing (EMDR), compassion-focused therapy and mindfulness have yet to show consistent benefit.
- Medication has a very limited role. Antidepressants may be helpful for co-existing depression, but do not treat prolonged grief disorder itself. Benzodiazepines are not recommended because of the risks of dependence and their potential to interfere with the learning and memory processes needed for adaptation.
(BMJ 2017;357:j2016, NEJM 2024;391:1227, Lancet 2025;405:1621)
Referral
- Consider referral to specialist mental health services when grief symptoms persist beyond 6–12 months and significantly impair functioning.
- Earlier referral can be considered if there is co-existing depression, post-traumatic stress, major role impairment, substance misuse or suicidal ideation.
Children and prolonged grief disorder
- Rates of prolonged grief disorder are around 5–10% in children.
- Features in children are often similar to those in adults, but are expressed in an age-appropriate manner – for example, a young child might persist in being obsessed with death-related play.
- In children who have lost a parent, the Family Bereavement Programme (that aims to build resilience in the child) has been shown to reduce immediate and long-term emotional problems, but access to this intervention is currently very limited.
- CBT has been shown to be beneficial in children with prolonged grief disorder.
Grief and other mental health conditions
Prolonged grief disorder is linked to poor physical health, suicidality, reduced quality of life and functional impairment. It is distinct, but has a high comorbidity rate with depression and PTSD. Bereavement can also trigger mental health problems such as depression, which may be difficult to distinguish from early grief, as well as anxiety disorders, alcohol or substance misuse and episodes of mania (BMJ 2017;357:j2016; BMJ 2017;358:j2854).
Grief and depression
- Grief is typically characterised by intense yearning or longing for the deceased. Symptoms are often most severe when the person is thinking about their loss. Unlike depression, people who are grieving may still experience moments of positive emotion, and often seek the company of others.
- In depression, pleasure and positive affect are persistently diminished. Social withdrawal is more common, and symptoms are not limited to reminders of the deceased.
- According to DSM-5 (APA, 2022), major depression can be diagnosed from two weeks after a bereavement if full criteria are met. Clinicians should then consider whether careful watchful waiting is appropriate, or whether active treatment is needed in the presence of suicidal thoughts, major role impairment or marked clinical deterioration.
Grief and trauma
PTSD can arise after bereavement, particularly when the death is sudden, violent or perceived as preventable. Both prolonged grief disorder and PTSD may follow loss, but they are distinct conditions.
- Prolonged grief disorder involves persistent yearning and preoccupation with the deceased, usually linked to separation distress, and often accompanied by bittersweet memories.
- PTSD symptoms are driven by traumatic distress, with intrusive memories, nightmares, flashbacks, hypervigilance and avoidance, often centred on the circumstances of the death.
- The two may overlap, especially after sudden or violent loss, but require different treatment approaches.
Unlike prolonged grief disorder, where referral is usually indicated only once disabling symptoms continue beyond 6–12m, PTSD can be diagnosed after just 1m. NICE (NG116, 2018) recommends referral for psychological assessment and treatment of PTSD if symptoms are severe, persist beyond 4w or cause significant functional impairment.
In primary care, it is therefore important to actively consider trauma following bereavement, and to assess for PTSD symptoms, because timely recognition and early referral may be crucial in preventing further deterioration.
(BMJ 2017;357:j2016, BMJ 2017;358:j2854, Lancet 2025;405:1621)
Supporting clinicians through grief
Grief is a significant and important experience that can have a major impact on clinician wellbeing. However, recognising and acknowledging the emotional effects early can help to reduce the risk of distress building up over time.
Some simple, practical steps include (Health Serv Insights 2025;18:11786329251344772):
- Seek support from colleagues: our team is often the most meaningful source of support, especially after a loss at work. Checking in regularly with each other and giving space to talk after a difficult death – even briefly – can help to reduce feelings of loneliness, guilt or self-doubt. If it seems likely that an event will affect someone more deeply, plan a follow-up conversation later in the day or week.
- Create small pauses after challenging cases: busy workloads or rapid transitions between patients can get in the way of natural processing of grief. Even one or two minutes to pause and reflect can help clinicians start to make sense of what happened. This might involve a quiet moment outside, taking a few slow breaths while making a drink, or a few simple grounding techniques to regain emotional stability before moving on to the next patient. Our article, Notice the NOW, highlights a simple tool for coping with distressing thoughts or emotions.
- Connect with family and friends: time with friends, family and loved ones outside work can offer warmth, perspective and a sense of normality, as well as reassurance and a sense of connection. It is often best to avoid detailed discussion of specific cases outside the workplace because colleagues who share our clinical context are better placed to provide detailed case-specific support. However, shared activities, light conversation or simply spending time with people who care about us can ease the emotional impact of a difficult day.
- Seek formal support when needed: this might include a debrief with a colleague or supervisor, a planned discussion at the end of the day, or accessing local psychological or mental health support if grief becomes persistent or starts to interfere with work.
|
Grief
|
|
|
Useful resources for patients: Websites (all resources are hyperlinked for ease of use in Red Whale Knowledge) Bereavement support organisations:
Information about grief:
Useful resources for clinicians: |
This information is for use by clinicians for individual educational purposes, and should be used only within the context of the scope of your personal practice. It should not be shared or used for commercial purposes. If you wish to use our content for group or commercial purposes, you must contact us at sales@red-whale.co.uk to discuss licensing, otherwise you may be infringing our intellectual property rights.
Although we make reasonable efforts to update and check the information in our content is accurate at the date of publication or presentation, we make no representations, warranties or guarantees, whether express or implied, that the information in our products is accurate, complete or up to date.
This content is, of necessity, of a brief and general nature, and this should not replace your own good clinical judgment or be regarded as a substitute for taking professional advice in appropriate circumstances. In particular, check drug doses, side effects and interactions with the British National Formulary. Save insofar as any such liability cannot be excluded at law, we do not accept any liability for loss of any type caused by reliance on the information in these pages.
Here is the link to our terms of use.