
This Pearl is provided as free content. Here is the link to our terms of use
Heat-related illness
Heat-related illness
Heat-related illnesses are a growing problem worldwide due to an increase in extreme heat events, and have been the subject of several reviews which may be helpful to us in primary care (NEJM 2019;380:2449, BMJ 2022;378:e070762, NEJM 2022;387:1404).
In the 20 years from 2002 to 2022, there was a 54% increase in heat-related mortality in people aged >65y (NEJM 2022;387:1404). When we think of heat illness, we might consider heatstroke to be our biggest concern, but other conditions can also be exacerbated by increased temperatures – such as IHD, renal and respiratory disease, and mental health conditions. In addition, a number of medications may increase the risk of heat-related illness. Our role in primary care might include both the recognition and management of heat-related illness, and taking action to reduce the risk in our more vulnerable patients.
This article was updated in January 2026.
Vulnerability to heat illness
Vulnerability to heat illness might result from external factors such as exposure to heat (outdoor workers/athletes), socioeconomic factors (access to cool spaces, ability to relocate if needed, social isolation) and individual factors that increase susceptibility (BMJ 2022;378:e070762, NEJM 2022;387:1404).
Those at increased risk include:
- The elderly (mortality can be >50% (NEJM 2019;380:2449)).
- Pregnant women.
- Pre-pubertal children.
- Athletes.
- Outdoor workers.
- Patients with chronic conditions.
- Patients who are socially isolated, or those with a history of substance misuse disorder.
- Those on certain medications, including diuretics, antidepressants, anticholinergics, antihypertensives, antipsychotics, lithium (NEJM 2022;387:1404).
Classification
Heat illnesses are classified into 2 subtypes:
- Classic heat illness:
- Due to excessive environmental heat and poor ability to dissipate that heat (NEJM 2019;380:2449).
- Affects our vulnerable patient groups.
- Mortality if not promptly treated is as high as 80% (NEJM 2022;387:1404).
- Exertional heat illness:
- IMPORTANT! High environmental temperature NOT required: physical exertion causes excess metabolic heat which overwhelms usual compensatory mechanisms.
- Affects soldiers, firefighters, agricultural workers, athletes, festival-goers (alcohol/drugs increase the risks).
- Can occur within 60mins of starting exercise, even if done same activity before without problems.
- Mortality up to 33% (NEJM 2022;387:1404).
The spectrum of heat illness
The BMJ reminds us that not all heat illness is heatstroke, and that determining the severity of the illness helps us decide what treatment is needed and how urgently (BMJ 2022;378:e070762).
| Severity | Heat-related condition | Pathology |
| Mild | Heat cramp | Painful muscle spasm in arms, abdomen or legs following activity. |
| Heat rash | Blockage of sweat glands leads to pruritic superficial vesicular rash. | |
| Moderate | Heat exhaustion |
Core body temperature is normal or only mildly increased. Fatigue, weakness, nausea, headache, faintness, clammy skin. |
| Heat syncope |
Syncope due to pooling of blood after standing immobile in heat. Diagnosis of exclusion. |
|
| Severe | Heatstroke | A multisystem life-threatening condition, described below. |
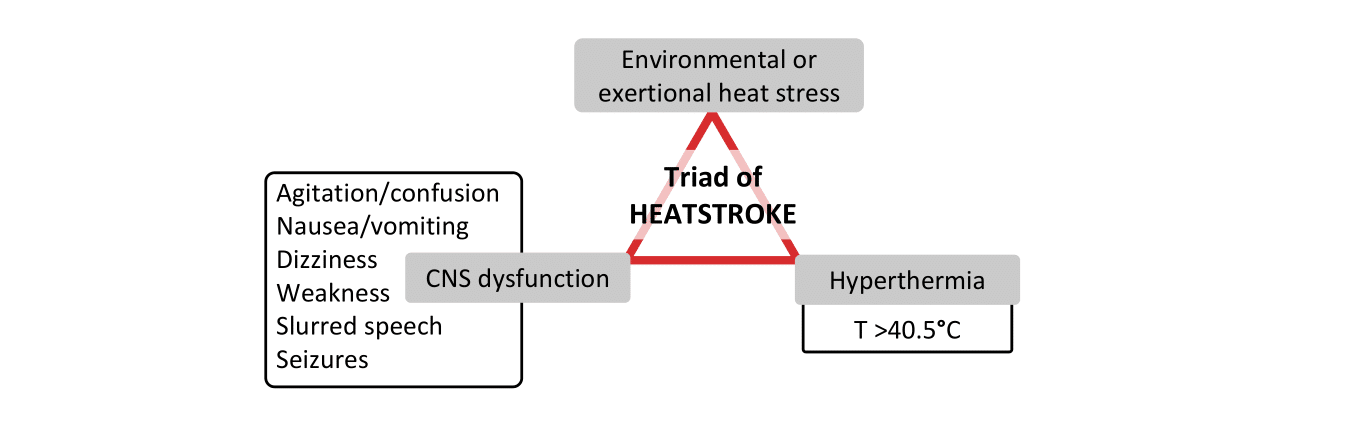
Heatstroke presentation
When the body’s compensatory mechanisms are overwhelmed:
- Rapid rise in core temperature.
- Fall in central venous pressure and cardiac collapse.
- Increased GI permeability, allowing toxins into the systemic circulation.
- Cell anoxia and inflammatory response.
This can lead to:
- Systemic inflammatory response syndrome (‘sepsis without the bacteria’).
- Multi-organ failure.
- CNS dysfunction.
Other symptoms:
- Flushed (excessive peripheral dilatation) or pale (circulatory collapse).
- Tachycardia, tachypnoea, hypotension.
- Profuse sweating and wet skin (in exertional heatstroke).
- Dry skin (in environmental heatstroke because sweat glands fail to respond).
Treatment
Severe heat illness
Very rapid cooling is the mainstay of initial treatment (the longer the body’s temperature is >40.5°C, the worse the prognosis) (NEJM 2022;387:1404). Start immediately while waiting for ambulance: delay only to do cardiopulmonary resuscitation!
- Immersion in ice cold water is the treatment of choice. This is unlikely to be available in primary care (!), but may be available at sporting events.
- If not available, pour copious amounts of water over the individual and fan them to increase evaporative loss (NEJM 2019;380:2449).
In the elderly with environmental heatstroke, ice packs, wet packs and fans may be better tolerated, but less effective at achieving rapid heat loss. Infusions of ice-cold fluids are also used, but are unlikely to be available in primary care!
Moderate heat illness
- External cooling measures such as ice packs in axillae and groins (BMJ 2022;378:e070762).
- Rehydration with oral fluids and electrolytes as needed.
- Monitor condition.
Mild heat illness
- Loosen clothing and allow evaporative cooling (BMJ 2022;378:e070762).
- Oral rehydration.
- Corticosteroid creams for itch if needed.
Heat-related illness in athletes
Heat-related illness in athletes occurs at higher ambient temperature and humidity, with one systematic review reporting rates of 4 cases per 1000 athletes in training and up to 6–7% of athletes in competition endurance running events (JAMA 2024;332:664). The authors identified key factors in prevention, which we at Red Whale feel could be applied more widely to any planned exertion at higher temperatures:
- Suspend or schedule breaks in events if the temperature is ≥32.2°C ‘wet-bulb globe temperature’, which measures heat stress risk using air temperature, humidity, wind and solar radiation factors (normal air temperature is measured with ‘dry-bulb globe temperature’). There are calculators online to help you work this out (Omni Calculator – wet bulb calculator).
- Mitigate risks by changing timing and location of events.
- Acclimatisation: training for 7–14 days prior to the event under similar conditions.
- Clothing: light-weight, loose-fitting, moisture-wicking fabrics.
- Hydration: individualised hydration planning, which may require post-exercise rehydration of 100–150% of fluid losses.
Occupational heat-related illness
Over an 11-year period in the USA (2011–2022), almost 500 people died from occupational-related heat exposure (JAMA 2025;334:267). Sadly, these deaths should be preventable. A JAMA Insight article highlighted that (JAMA 2025;334:267):
High-risk workplaces include:
- Outdoors: agriculture, grounds keepers, construction, postal workers, transport workers, disaster clean-up.
- Indoors: kitchen or warehouse workers, foundry workers, miners.
The risks come from:
- High ambient temperature (e.g. from the sun, hot equipment).
- Heat generation from physical effort, and difficulty cooling because of PPE.
- Insufficient rest breaks/access to water to rehydrate.
- Lack of heat acclimatisation (takes 2 weeks to acquire, lost after about 1 week).
Legislation should offer some protection to workers, but clinicians can raise awareness of the issues and encourage workers to seek appropriate advice (e.g. involving unions).
A drop in the ocean
Acute heat-related illnesses account for only a fraction of the overall health burden of extreme heat (NEJM 2024;390:1793). Evidence from epidemiological studies links heat with increased rates of a broad range of other conditions, including:
- Cardiovascular events and death, including myocardial infarction, arrhythmias, heart failure and stroke.
- Exacerbation of asthma or COPD.
- Complications of diabetes.
- Exacerbation of kidney disease.
- Adverse pregnancy outcomes, including preterm delivery, stillbirth, miscarriage and low birth weight.
- Suicidality, aggressive behaviour and violence.
- All-cause hospital admission.
Those at highest risk include older people, those with multimorbidity, ethnic minority groups and those with lower socioeconomic status. Further research is needed into the effects of increased heat on health, and strategies for mitigation and improved resilience, particularly among high-risk groups.
|
Heat-related illness
|
|
| Consider identifying patients vulnerable to heat illness in your practice, and providing information on recognition and avoidance at their next annual review. |
This information is for use by clinicians for individual educational purposes, and should be used only within the context of the scope of your personal practice. It should not be shared or used for commercial purposes. If you wish to use our content for group or commercial purposes, you must contact us at sales@red-whale.co.uk to discuss licensing, otherwise you may be infringing our intellectual property rights.
Although we make reasonable efforts to update and check the information in our content is accurate at the date of publication or presentation, we make no representations, warranties or guarantees, whether express or implied, that the information in our products is accurate, complete or up to date.
This content is, of necessity, of a brief and general nature, and this should not replace your own good clinical judgment or be regarded as a substitute for taking professional advice in appropriate circumstances. In particular, check drug doses, side effects and interactions with the British National Formulary. Save insofar as any such liability cannot be excluded at law, we do not accept any liability for loss of any type caused by reliance on the information in these pages.
Here is the link to our terms of use.