 Chronic heart failure
Chronic heart failure
-
1. Chronic heart failure
- 1.1 Headlines
- 1.2 Inequalities in chronic heart failure
- 1.3 Epidemiology
- 1.4 Causes
- 1.5 Terminology
- 1.6 Diagnosis of chronic heart failure
- 1.7 Heart failure with preserved ejection fraction (HFpEF): suspecting and diagnosing
- 1.8 Management of heart failure
- 1.9 Management of heart failure with reduced ejection fraction (HFrEF)
- 1.10 HFpEF management: the twin pillar house
- 1.11 Evidence for drugs used in HFpEF
- 1.12 Medication in heart failure management: starting and monitoring
- 1.13 Cardiac rehabilitation
- 1.14 Chronic heart failure reviews
- 1.15 Palliative care
- 1.16 Dilemmas in chronic heart failure
This Pearl is provided as free content. Here is the link to our terms of use
Chronic heart failure
Chronic heart failure
Heart failure is the clinical manifestation of impaired cardiac function. It is often due to impairment of the left ventricle (either weakness or impaired relaxation), but may result from issues with the right ventricle, valves or pericardium (NICE 2025, NG106).
This article covers chronic heart failure (CHF). Guidance on acute heart failure (NICE 2014 (updated 2021), CG187) focuses on hospital management and is not summarised here.
A new diagnosis of heart failure carries a prognosis similar to many cancers, with around a 50% chance of death within 5 years, (Eur J Heart Fail 2021;23:1514).
This article was last reviewed in March 2026.
| Glossary and abbreviations | |
| HFrEF | Heart failure with reduced ejection fraction |
| HFpEF | Heart failure with preserved ejection fraction |
| HFmrEF | Heart failure with mildly-reduced ejection fraction |
| LVEF | Left ventricular ejection fraction |
| MRA | Mineralocorticoid receptor antagonist |
| SGLT2i | Sodium–glucose cotransporter 2 inhibitor (the -gliflozins) |
| ARNI | Angiotensin receptor neprilysin inhibitor (e.g. Entresto) |
Headlines
If you have only a couple of minutes to spare, here are the headlines from NICE 2025, NG106:
- NICE recognises ‘mildly-reduced ejection fraction heart failure’ (LVEF 41–49%) as a separate entity, bringing it into line with other major guidelines.
- The guideline encourages us to be more proactive, aggressive and collaborative than previously, with the hospital MDT playing a leading role, especially following diagnosis.
Management includes:
- ‘Quadruple therapy’ for HFrEF (‘offer’) and HFmrEF (‘consider’) at diagnosis.
- ‘Dual therapy’ for HFpEF: MRA + SGLT2i.
- SGLT2i drugs (the ‘gliflozins’) are recommended across all types of heart failure. The ‘specialist initiation only’ restriction for SGLT2i has been removed for HFrEF (but remains for HFmrEF and HFpEF).
- ARNIs (e.g. Entresto) are recommended in some circumstances to treat HFrEF, usually on the advice of a heart failure specialist.
- IV iron therapy for some with HFrEF.
- Blood monitoring: recommendations for starting and uptitrating ACEi, ARB, ARNI and MRAs have been unified and simplified.
Inequalities in chronic heart failure
Socioeconomic deprivation
UK-based population studies using the Clinical Practice Research Datalink (CPRD) show that socioeconomically disadvantaged people are more likely to develop heart failure and have more comorbidities than affluent people. Additionally, those from lower socioeconomic backgrounds develop heart failure at a younger age. This socioeconomic inequality widened between 2002 and 2014 (Lancet 2018;391:572).
Ethnicity
Racial differences in heart failure
Data from the USA suggests that Black people have higher rates of risk factors for heart failure (hypertension and type 2 diabetes) than White people. Black people are more likely to develop heart failure if exposed to the same risk factors (Circulation 2023;148:220).
Do Black patients get less benefit from ACEi/ARB drugs in HFrEF?
No. A meta-analysis of 16 000 patients (over 5 trials) found that the mortality benefit of these drugs was similar between Black and other ethnicities (JAMA 2024;331:2094).
Under-representation of minority groups in heart failure trial data
Clinical trials may under-represent people from certain groups: females, older adults and ethnic minorities (Eur. Heart J 2023;44:921).
Ethnicity: a minority of trials report race and ethnicity data. In those that do, Black, Indigenous and people of colour were under-represented relative to disease distribution (Circ Heart Fail 2022;15:e008685).
Geographic distribution: countries with higher heart failure prevalence are under-represented in trial collaboration and enrolment. Trial diversity would improve if more research was undertaken outside Europe and North America (EHJ Qual Care Clin Outcomes 2022;8:659).
Sex: females are under-represented in clinical trials of heart failure with reduced ejection fraction (Eur J Heart Fail 2021;23:15).
Older adults: most hospitalised older patients would not meet enrolment criteria for inclusion in clinical trials, and these ‘typical’ heart failure patients are likely under-represented (Am Heart J 2003;146:250).
Epidemiology
The prevalence of heart failure at age <55y is <1%, rising to over 10% for those aged ≥70y.
The average age at diagnosis is 76y (NICE 2025, NG106).
Prevalence is rising. The age-adjusted incidence of heart failure appears to be falling (maybe due to improved management of CVD), but the overall incidence is rising due to the ageing population (EHJ 2021;42:3599).
In the UK, around 1 million people have heart failure, with 200 000 new diagnoses annually (NICE 2025, NG106). There is a slight female preponderance in prevalence (EHJ 2021;42:3599).
We have previously thought that around 50% of patients have reduced ejection fraction heart failure and 50% have preserved ejection fraction heart failure, but these trials were hospital based. Community studies now suggest that 60% have HFrEF, 24% HFmrEF and 16% HFpEF (EHJ 2021;42:3599).
Causes
In the developed world, the two main causes of CHF are hypertension and ischaemic heart disease (IHD).
Other causes include (EHJ 2021;42:3599):
- Valve disease.
- Congenital heart disease.
- Arrhythmias.
- Cardiomyopathy.
- Infective (myocarditis, HIV, Lyme disease).
- Infiltrative, e.g. amyloid.
- Drug induced, e.g. anthracyclines (the ‘-rubicin’ chemotherapies).
- Storage disorders (haemochromatosis, Fabry disease, glycogen storage diseases).
- Neuromuscular disorders (Friedreich’s ataxia, muscular dystrophy).
- Pericardial, e.g. calcification.
Terminology
Heart failure is divided into different types according to ejection fraction. Ejection fraction is the amount of blood (%) pumped out of the ventricle between the end of diastole and the end of systolic contraction.
Heart failure with preserved ejection fraction (HFpEF): left ventricular ejection fraction (LVEF) of ≥50%, plus 2 or more ‘structural issues’.
NICE provides a list, but these are echo findings and thus not relevant to most of us in primary care. Broadly, they measure left atrial volume, left ventricular wall thickness (a measure of LVH), pulmonary artery pressure and the ratio of mitral valve flow velocities (see NICE 2025, NG106 ‘Terms used in this guideline’ for the numbers!).
Heart failure with mildly-reduced ejection fraction (HFmrEF): LVEF 41–49%.
Heart failure with reduced ejection fraction (HFrEF): LVEF ≤40%.
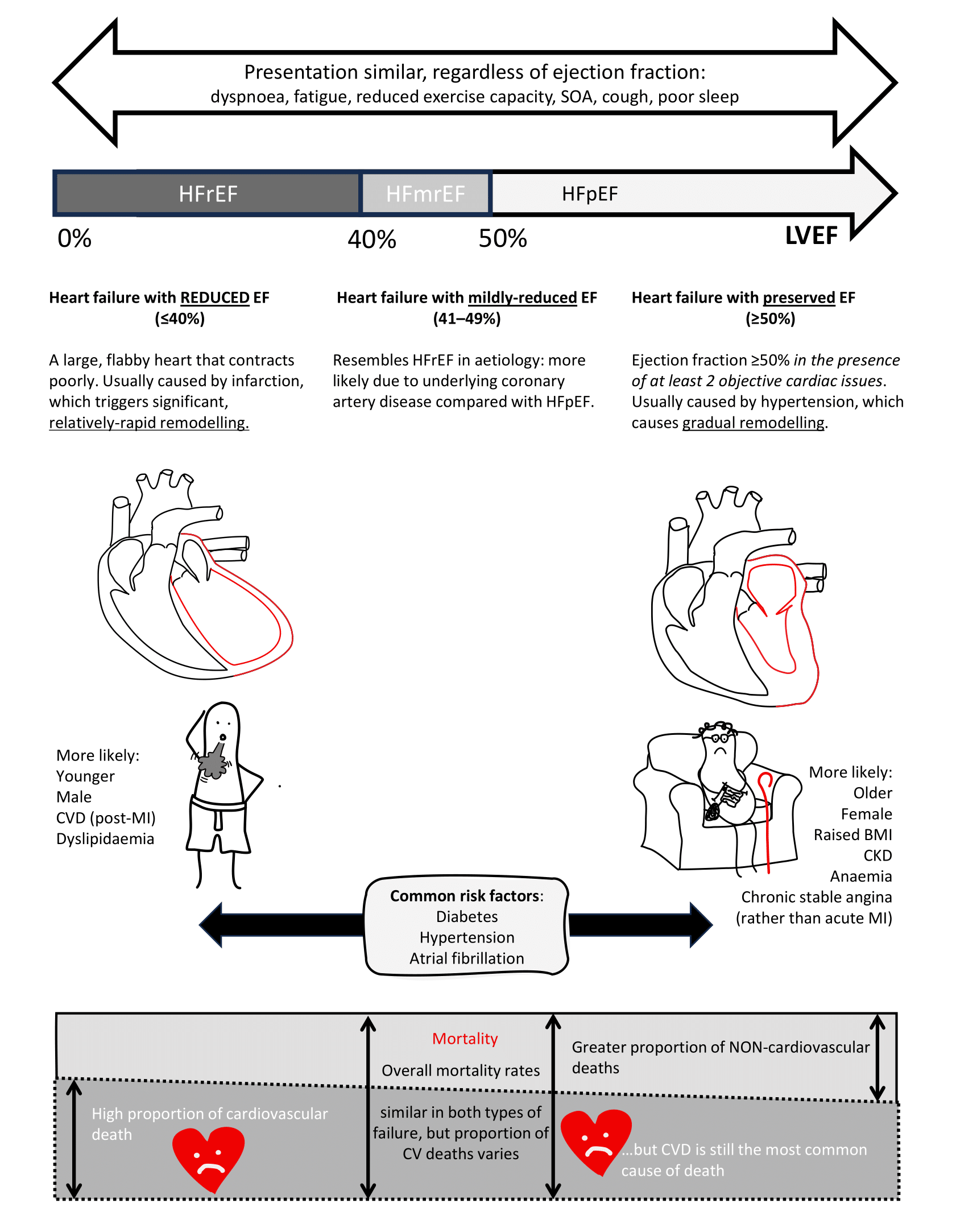
Image: summarises the key differences between the types of heart failure (Front Cardiovasc Med 2021;8:678121, Lancet 2024;403:1604, BJGP 2024;74:103).
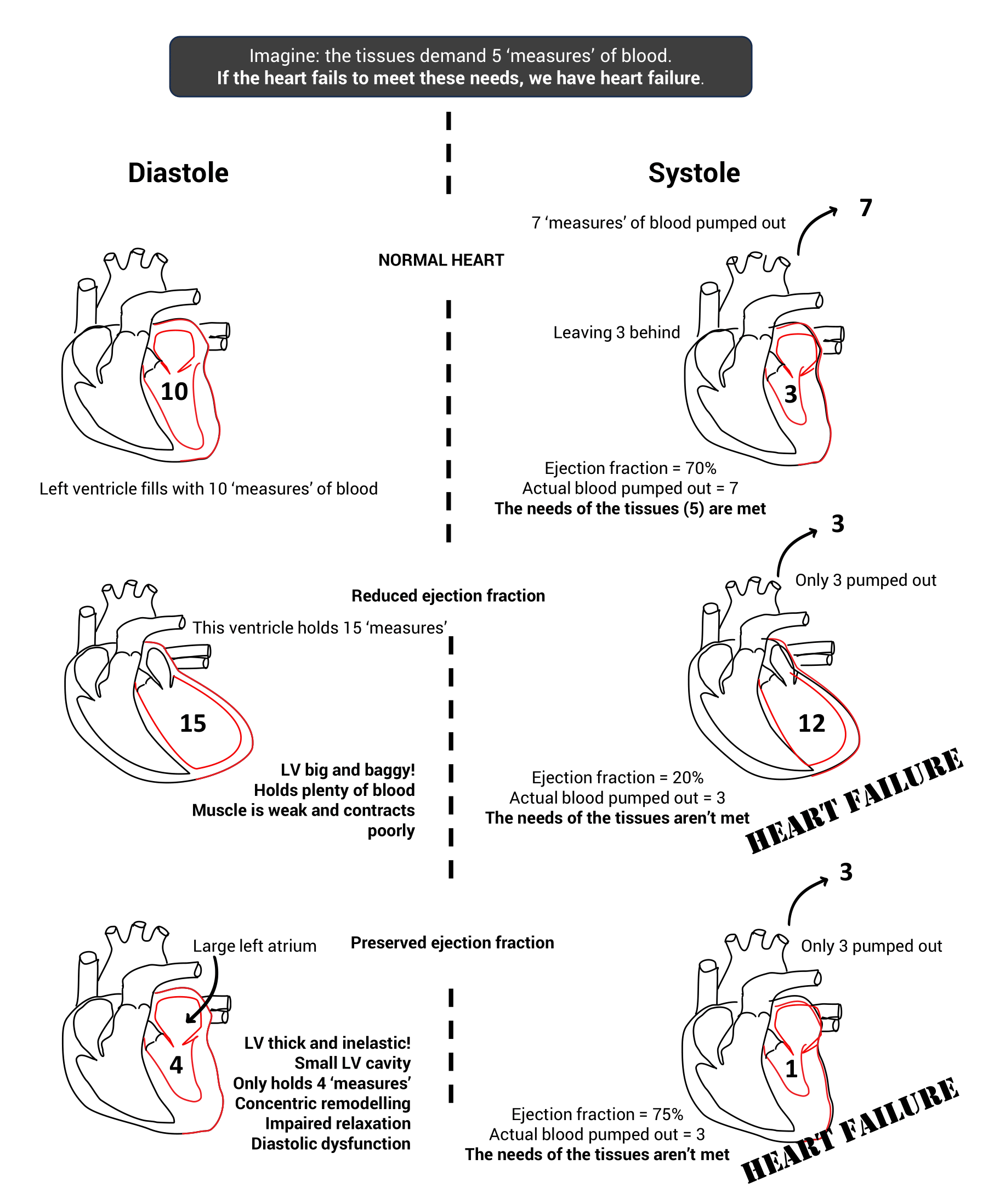
How can a person have heart failure with a normal ejection fraction?
Diagnosis of chronic heart failure
Coding
Coding ‘heart failure with preserved ejection fraction’ is rarely done in general practice. Improved coding would aid management of HFpEF, reduce ineffective prescribing and help recruitment into future studies (BJGP 2024;74:103). Beware of using the functional NYHA breathlessness codes in other conditions, e.g. COPD, because your patient may end up on the heart failure register!
Earlier diagnosis
A BJGP editorial discussed the need for earlier diagnosis (BJGP 2023;73:4). Two things hamper this:
- The public do not recognise the symptoms or they attribute them to ‘old age’, hence the BEAT-HF campaign: Breathless, Exhausted, Ankle swelling? Time for a simple blood test.
- When people present, their symptoms are often attributed to pre-existing disease.
Given that the first step is a simple blood test, reflecting on your practice, could you look for heart failure more often?
What about screening?
This isn’t recommended in current guidelines, but a Dutch group found that in older patients with hypertension, raised BNP predicts future cardiovascular events (especially heart failure) and all-cause mortality. This 9-year prospective cohort study of 530 patients aged 60–85y found that BNP was a better predictor than ECG and echocardiogram (BJGP 2024;74:e219).
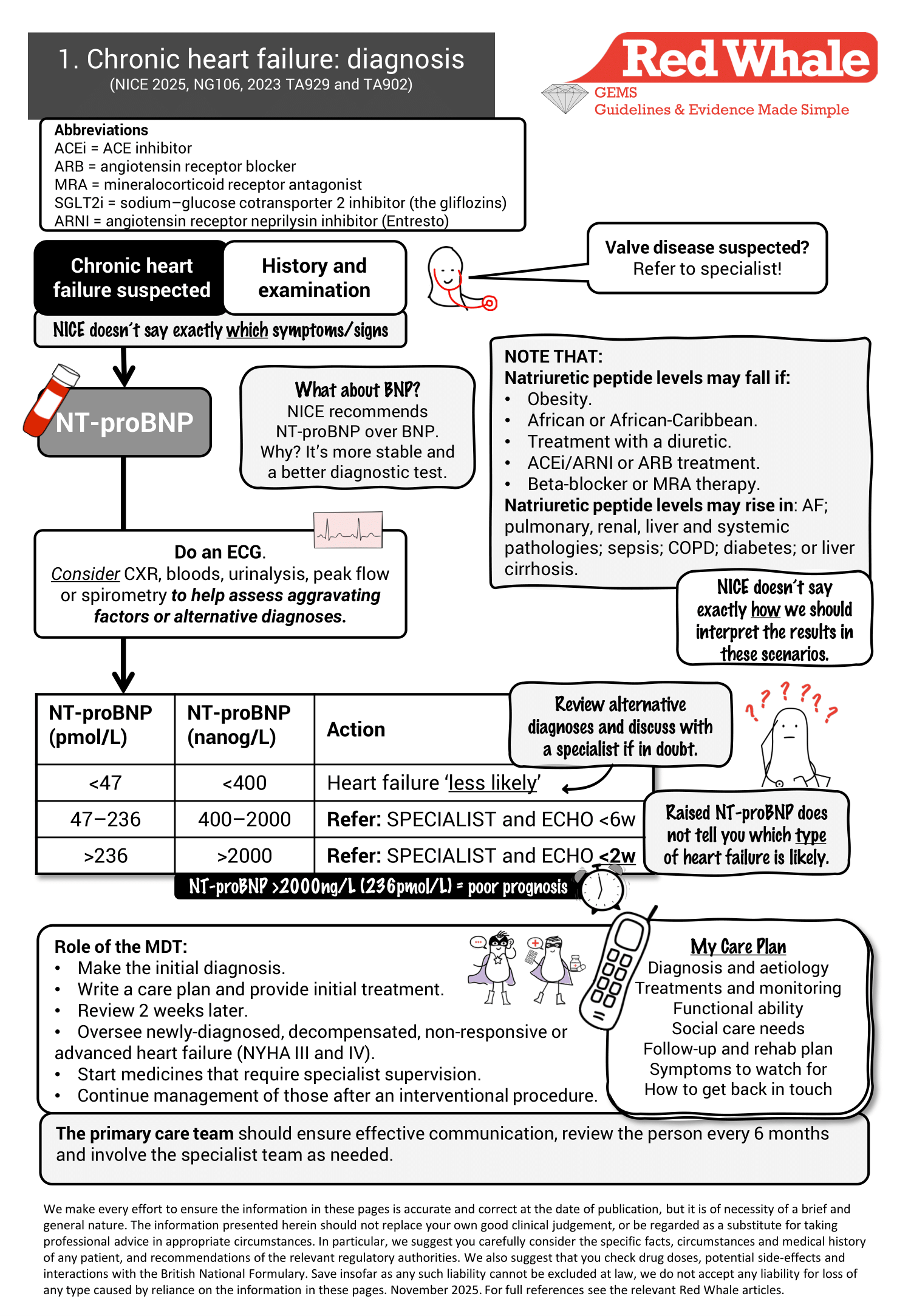
What are natriuretic peptides?
Natriuretic peptides are released during cardiac wall stress and are cardioprotective. The precursor proBNP splits into a biologically active peptide called BNP and an inert peptide called NT-proBNP (N-terminal proBNP). Both BNP and NT-proBNP rise in heart failure (SIGN 2016, 147, Pharmacol Ther. 2021;227:107863).
BNP is an angiotensin II antagonist causing diuresis, vasodilatation and inhibition of aldosterone secretion.
NT-proBNP is more stable and more sensitive than BNP.
Atrial fibrillation can raise NT-proBNP even in the absence of heart failure. The optimal threshold for NT-proBNP in atrial fibrillation is not known, and NICE has issued a research recommendation to answer this question (NICE 2025, NG106/3).
Note that NICE found ECG inferior to NT-proBNP as a diagnostic test, but ECG is felt to be an essential investigation in subsequent general assessment of suspected heart failure (SIGN 2016, 147).
Is the NT-proBNP cut-off set by NICE appropriate?
European thresholds are lower than NICE thresholds.
A study analysed UK primary care data from the CPRD database. It showed that (BJGP 2023;73:e1):
- By using European rather than NICE cut-offs (the European Society of Cardiology cut-off for NT-proBNP is ≥125 vs. NICE’s ≥400pg/ml), NICE misses 1 in 5 diagnoses of heart failure, but results in fewer referrals.
- If the European cut-off was used, for every 1 person diagnosed with heart failure, 20 would need to be referred for echo.
- Of note, a negative test (by either cut-off) was highly accurate (98% of those below the NICE cut-off did not have heart failure (this was 99% with the lower ESC cut-off).
What does this mean in practice?
The level of NT-proBNP cut-off is a balance between picking up those with heart failure vs. the economic (and personal) costs of over-investigating, and is decided at a national level.
The authors conclude that nearly all patients with a negative level did NOT have heart failure, but if someone has classic symptoms and signs of heart failure, it is still possible that they have heart failure. NICE suggests seeking specialist advice in this situation.
Heart failure with preserved ejection fraction (HFpEF): suspecting and diagnosing
What causes HFpEF?
The key risk factors and pathological processes are summarised below (Lancet 2024;403:1083 and JAMA 2023;329:827).
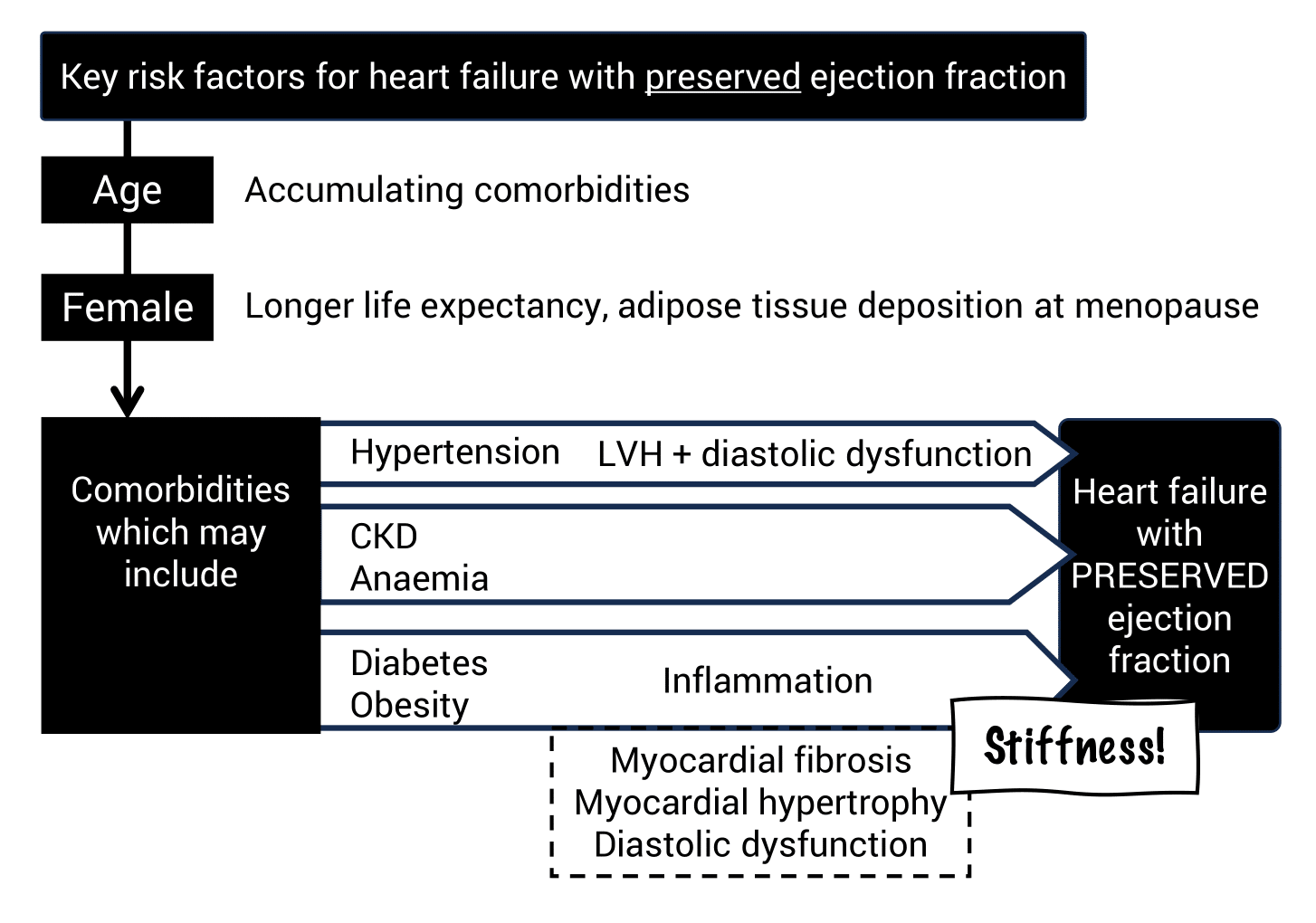
Diastolic dysfunction is key in developing HFpEF: impaired relaxation causes increased filling pressures at rest or exertion. Several other contributing factors may be present (not on the diagram), including slight LV systolic dysfunction, LA remodelling and impairment, pericardial restraint, pulmonary hypertension and systemic vascular stiffening.
Menopause may also contribute due to increased epicardial adipose tissue, which adds to diastolic dysfunction (Int J Cardiol 2024;415:132478).
Diagnosis of HFpEF in the community may be challenging.
How should we approach this ‘easy to miss’ diagnosis in practice? There are 3 key steps (Lancet 2024;403:1083):
- Clinically suspect heart failure:
- The commonest symptom is breathlessness on exertion and reduced exercise capacity: ask particularly about change in exercise capacity over time.
- Fluid overload is common, but may be absent, especially if diuretics are already being taken for hypertension. This makes the condition easy to overlook.
- Beware: a potential pitfall is that comorbidities may ‘explain away’ symptoms, e.g. COPD, obesity, advanced age, frailty and deconditioning.
- Find NT-proBNP ≥400:
- NT-proBNP ≥400 is usually seen in those with heart failure, but not always!
- 1 in 5 of those with HFpEF will have NORMAL natriuretic peptide.
- Echo confirmation with specialist interpretation:
- The left ventricular ejection fraction (LVEF – the only number other than heart rate most of us understand on the echo report!) will be preserved (≥50%).
- Hopefully, the report will say (in big letters): THIS IS HEART FAILURE WITH PRESERVED EJECTION FRACTION. It’s often not quite this clear, but a specialist referral should have taken place and they’ll check all the numbers.
Why might HFpEF lead to lower NT-proBNP levels?
- Natriuretic peptides are released due to high LV diastolic wall stress. Wall stress is inversely proportional to wall thickness, and mild LVH is common in HFpEF – this may reduce diastolic wall stress and reduce production of natriuretic peptide.
- Obesity (a key risk factor) also leads to lower natriuretic peptide levels due to increased expression of clearance receptors and peptide degradation by adipose tissue.
Pitfalls in diagnosis of HFpEF
- First pitfall: NT-proBNP is not 100% reliable as a rule-out test. If your patient looks like they have heart failure but the NT-proBNP is <400, they still might! Consider discussion with a specialist.
- Our second pitfall is requesting an echo but waiting to base the decision to refer on the result. Remember, the MDT will assess the patient, the blood results and the echo (alongside any other investigations), and they will decide whether your patient has heart failure or not. The danger is that we don’t refer, get the echo, find a normal LVEF, code it as ‘normal – no action’ then lose the patient to follow-up.
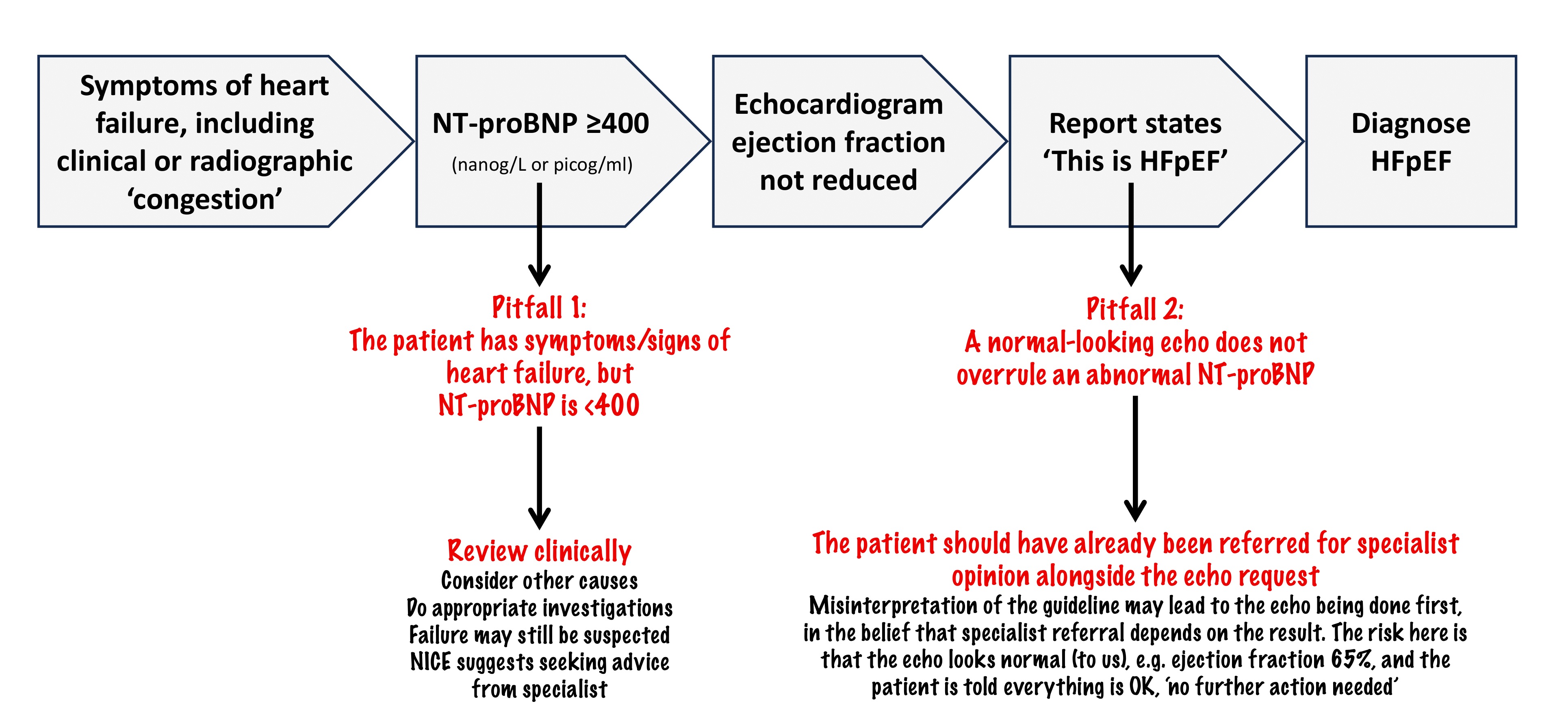
Due to this potential confusion over echocardiographic parameters, the authors of the Lancet review call for secondary care-based ‘heart failure diagnostic pathways’ that do everything (NT-proBNP measurement, ECG and echo) once clinical suspicion is aroused in primary care (Lancet 2024;403:1083).
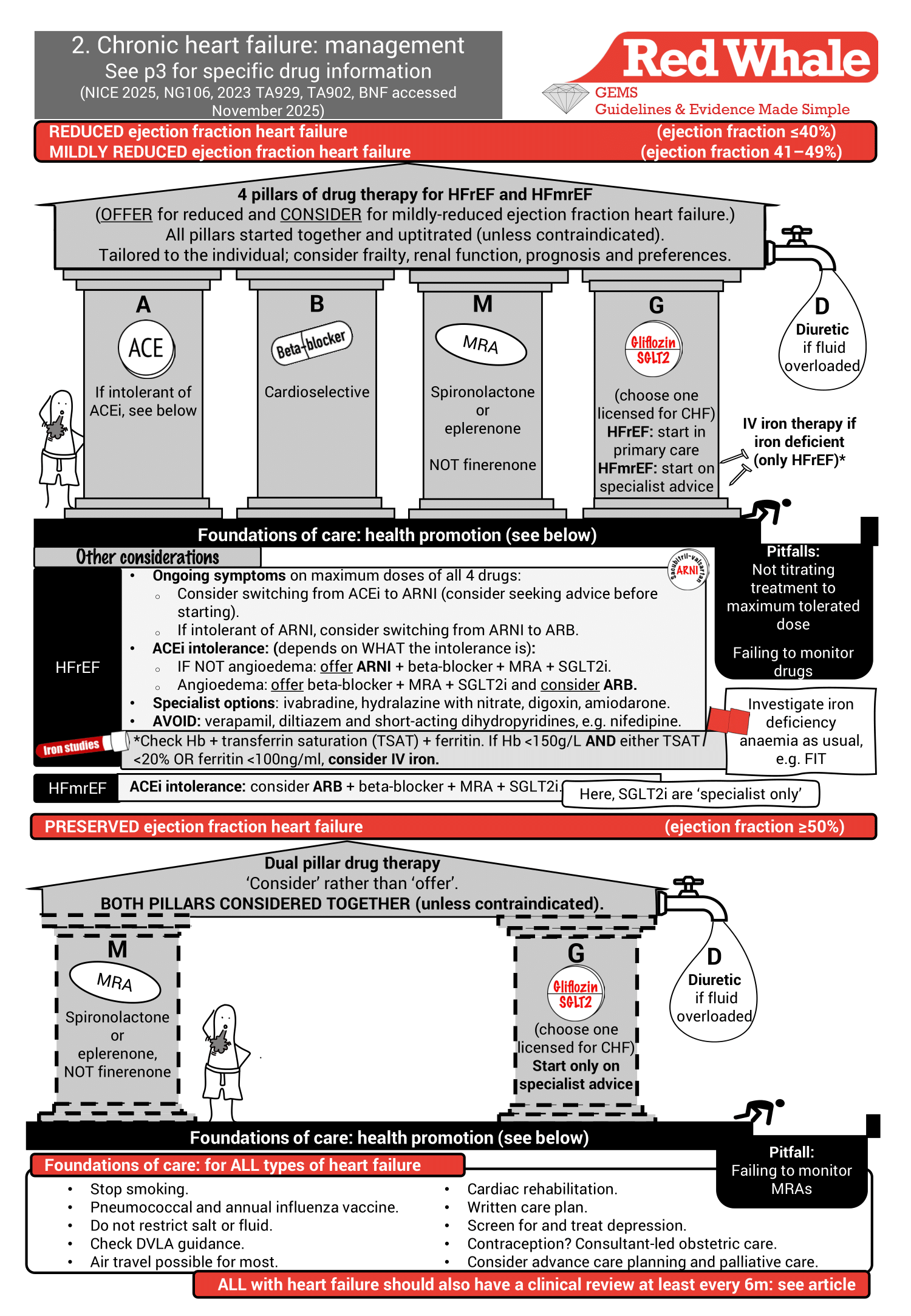
Management of heart failure
We summarise chronic heart failure management on page 2 of our GEMS:
Management of heart failure with reduced ejection fraction (HFrEF)
The importance of all 4 pillars in HFrEF
Does treatment make a difference? YES! Good treatment can make a massive difference. A network meta-analysis suggests that an ideal combination of drugs greatly reduces all-cause mortality (HR 0.39, 95% CI 0.31–0.49) and a composite endpoint of cardiovascular death or hospitalisation with heart failure (HR 0.36, 95% CI 0.29–0.46) (BMJ 2024;384:e077057).
Does it matter if we use only 1 or 2 of the medications from the 4 pillars? This diagram illustrates the striking cumulative benefits of the 4-pillar combination on all-cause mortality when compared with using just 1 or 2 agents (JACC Heart Fail 2022;10:73).
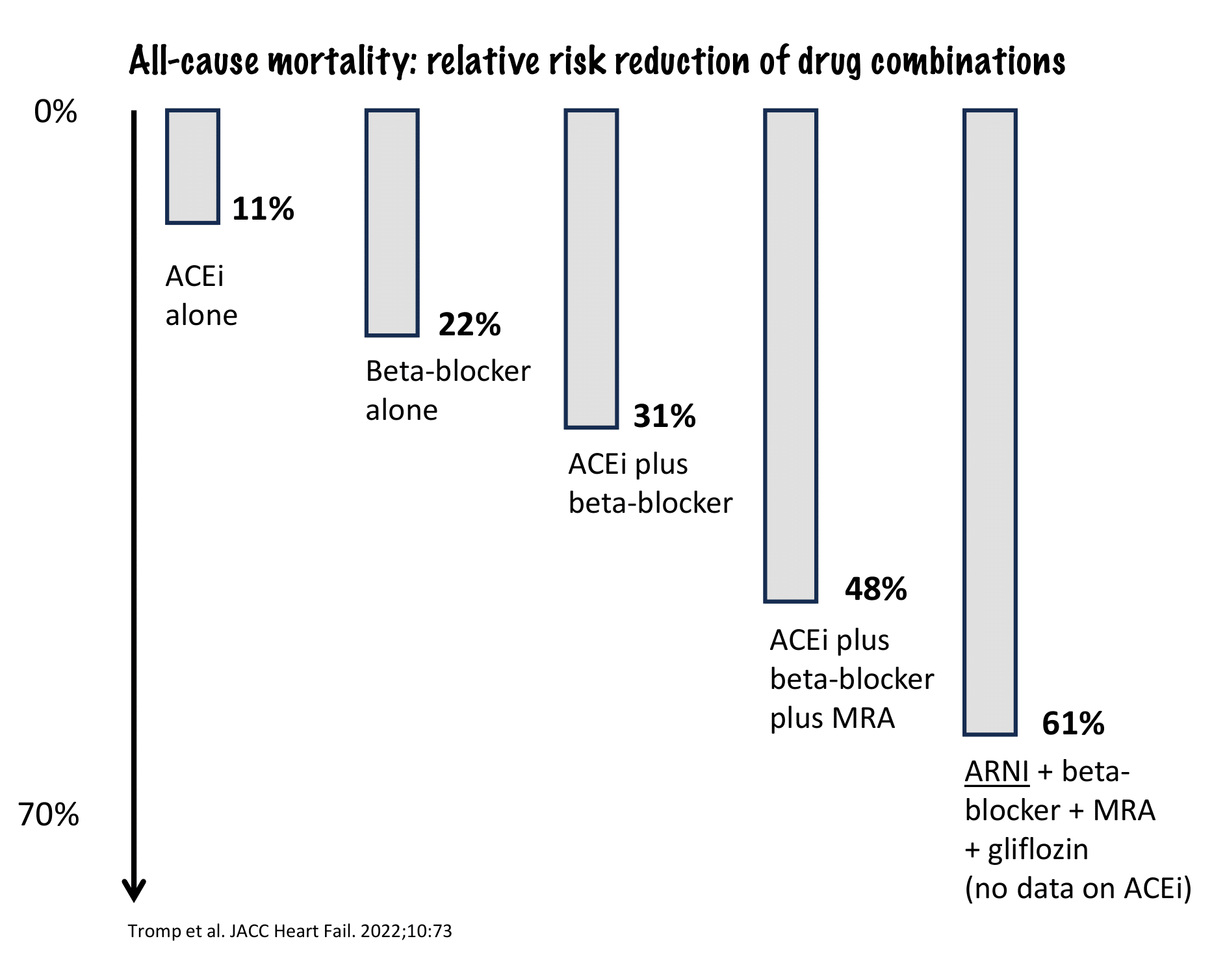
Note that the data did not include the combination of ACEi + beta-blocker + MRA + gliflozin. Instead, it used an ARNI drug, but this doesn’t change the base message that combinations appear to confer significant benefits.
Patients aged 55y with HFrEF on all 4 classes live over 6 years longer than those just taking ACEi + beta-blocker (DTB 2025;63:133).
The main barriers to achieving early and rapid quadruple therapy are low blood pressure, hyperkalaemia and CKD (Clin Med 2025;25:100296). Rapid initiation is more challenging in the presence of more severe heart failure alongside significant comorbidities.
Evidence for drugs used in HFrEF
Supporting evidence for ACEi and beta-blockers in HFrEF
Evidence supporting the use of ACEi and beta-blockers has been around for some time. ACE inhibitors were the first class of drug to show survival benefits in HFrEF (1980s and 1990s landmark trials included ATLAS, CONSENSUS and SOLVD).
- ACE inhibitors confer a 28% reduction in a composite endpoint of death, MI and hospital admission in those with LV dysfunction after MI (Lancet 2000;355:1575). ACEi provide increased efficacy at lower ejection fractions.
- Beta-blockers also reduce the relative risk of mortality in HFrEF by 35% (Eur J Heart Fail 2001;3:351):
- Absolute risk reduction in mortality over 12m is 5% (NNT 20).
- Absolute risk reduction of hospitalisation for heart failure over 12m is 5.7% (NNT 16).
Beta-blockers lower sympathetic activity, reducing vasoconstriction and myocardial stress. Lower catecholamine levels reverse remodelling and fibrosis (DTB 2025;63:133).
Supporting evidence for SGLT2i (gliflozins) in HFrEF
Glifllozins can be initiated in primary care for HFrEF. We should use a drug licensed for heart failure (currently dapagliflozin or empagliflozin).
The mechanism of action of gliflozins in heart failure is thought to be multifactorial: diuresis, anti-inflammatory action, improved myocardial and vascular metabolism (from glucose to ketone), reduced preload, reduced afterload and improvements in cardiac structure and function (American College of Cardiology, Focus on Heart Failure, accessed October 2025, DTB 2025;63:133).
Trials suggest that benefits of SGLT2i drugs are similar across all types of heart failure.
The key trials were DAPA-HF and EMPEROR-Reduced, but a Lancet meta-analysis looked at the benefits of dapagliflozin and empagliflozin across all types of heart failure (Lancet 2022;400:757). Compared with placebo, gliflozins:
- Reduced the composite endpoint (cardiovascular deaths/worsening heart failure): NNT 25 to reduce cardiovascular death or hospitalisation for heart failure over 23 months.
- Reduced admissions with heart failure: NNT 28 to reduce risk of first hospitalisation with heart failure over 23 months.
- Reduced cardiovascular death as a single endpoint: NNT 88 to reduce risk of cardiovascular death over 23 months.
- Reduced all-cause mortality: NNT 92 to reduce all-cause mortality over 23 months.
- Improved quality-of-life scores by around 20%.
Most of the patients in the trials had NYHA stage II failure, and benefit was seen to be slightly reduced (but still statistically significant) in patients with NYHA III or IV failure. No patients in the trials had an eGFR <20. Women were well represented, but Black and ethnic minority groups were relatively under-represented in the trials.
The DTB reminds us to use SGLT2i with caution in those age ≥85y due to limited safety data (DTB 2025;63:133).
Supporting evidence for IV iron in HFrEF
Iron deficiency is common in those with heart failure with reduced ejection fraction, especially if there is coexisting CKD. NICE made a recommendation for IV iron replacement in those with HFrEF and iron deficiency.
Check Hb, transferrin saturation (TSAT) and ferritin in heart failure (all types) and in those with HFrEF. If Hb <150g/L and either TSAT <20% or ferritin <100ng/ml, we are asked to ‘consider’ IV iron.
IV iron improved exercise tolerance and quality of life in the first year following treatment and was found to be cost-effective. It may also reduce hospitalisations for heart failure. (NICE 2025, NG106).
There was not enough evidence to support IV iron in those with HFmrEF or HFpEF (NICE 2025, NG106).
The guideline also reminds us to consider and investigate the cause of the iron deficiency. Do they need a FIT?
Oral iron is poorly absorbed in people with heart failure with reduced ejection fraction, and is not a substitute for IV iron. Oral iron performs no better than placebo in trials (NICE 2025, NG106).
Supporting evidence for MRA drugs in HFrEF
NICE does not recommend any particular MRA, but spironolactone and eplerenone are the likely choices (finerenone, a non-steroidal MRA, is limited by NICE to treat CKD in those with type 2 diabetes). Eplerenone is more specific in its action than spironolactone, and causes less gynaecomastia. The evidence shows that MRA drugs (EHJ 2021;42:3599):
- Substantially reduce mortality (30% reduction in risk of death; NNT 9, trial stopped early (RALES NEJM 1999;341:709)).
- Reduce admissions due to heart failure.
- Improve symptoms.
- Cause hyperkalaemia.
These outcomes are likely to result from their effects on reducing harmful cardiac remodelling and fibrosis, rather than their action as a diuretic (Int J Cardiol Heart Vessel 2014;3:6).
Supporting evidence for angiotensin receptor neprilysin inhibitors (ARNI) in HFrEF
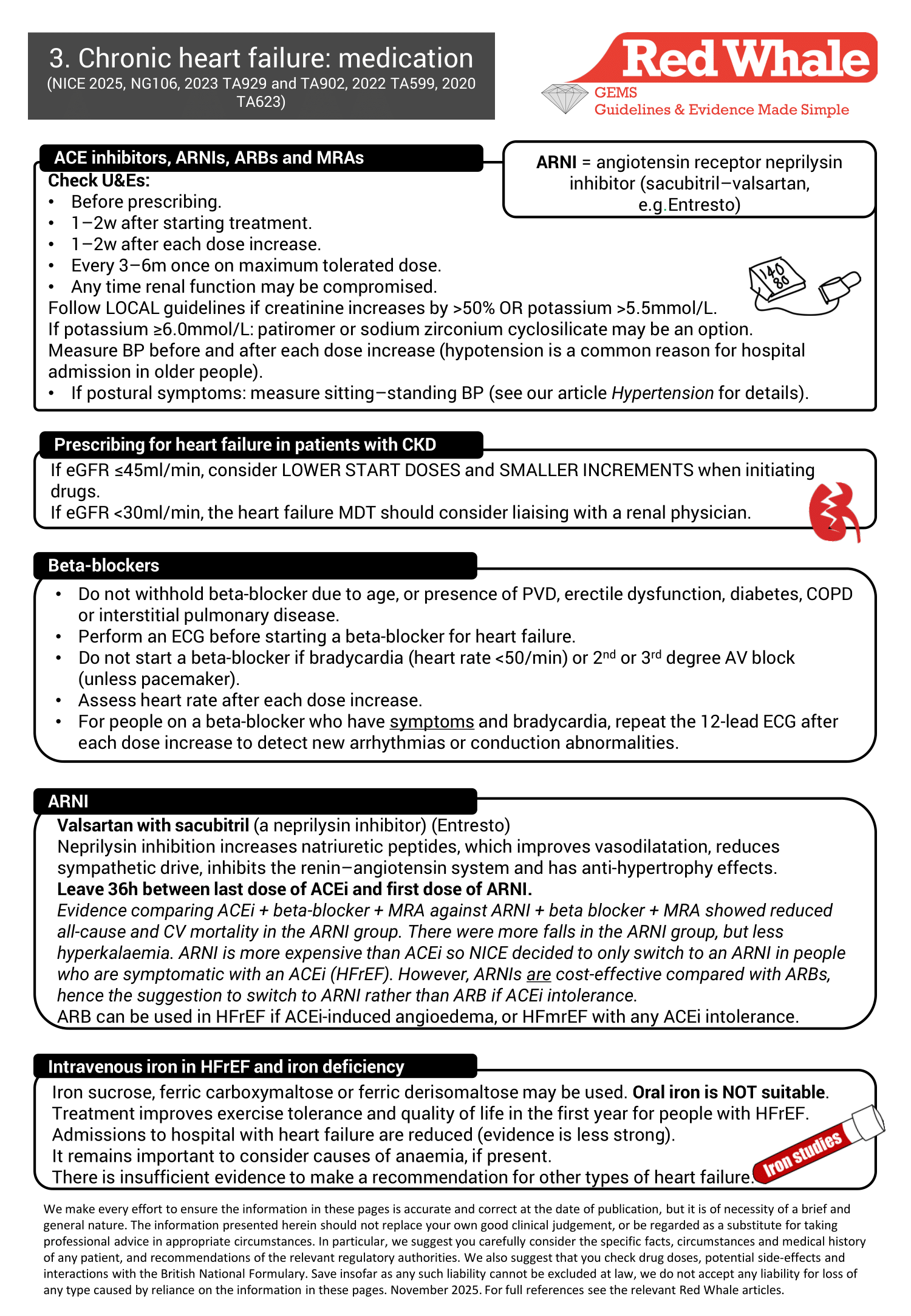
ARNIs are recommended by NICE for those with HFrEF who are intolerant of ACEi. They contain valsartan (an ARB) and sacubitril (a neprilysin inhibitor).
- They should not be given with an ACEi or ARB.
- NICE recommends 36h between the last dose of ACEi and the first dose of ARNI (NICE 2025, NG106).
- Once commenced, stopping an ARNI can cause a clinical deterioration (EHJ 2021;42:3599).
What is neprilysin!?
Neprilysin inhibition increases the concentration of natriuretic peptides, which:
- Improves vasodilatation.
- Reduces sympathetic drive.
- Inhibits the renin–angiotensin system.
- Has anti-hypertrophy effects.
What is the evidence?
When comparing ACEi + beta-blocker + MRA against ARNI + beta-blocker + MRA, after considering 28 trials, NICE concluded that all-cause and CV mortality were reduced in those in the ARNI group. There were more falls in the ARNI group, but fewer cases of hyperkalaemia.
HFpEF management: the twin pillar house
One of the most significant changes in the 2025 NICE guidance is considering dual therapy with an MRA and SGLT2i to treat HFpEF (NICE 2025, NG106). This is alongside diuretics (if fluid overloaded) and the other foundation treatments in our house of heart failure, common to all types of heart failure.
An article in the journal Heart discussed HFpEF (Heart 2023;109:874):
- Mortality is similar to those with reduced ejection heart failure (5-year mortality 50–70%).
- Rates of admission and hospitalisation are similar to those with other types of heart failure.
Until relatively recently, diuresis was the only treatment for HFpEF and the only drug treatment suggested in the previous iteration of the NICE heart failure guideline.
Evidence for drugs used in HFpEF
Supporting evidence for gliflozins in HFpEF
NICE signposts us to the two technology appraisals, TA902 and TA929 (NICE 2023, TA902 and TA929), which cover the recommendations and supporting evidence for dapagliflozin and empagliflozin when used for heart failure with preserved and mildly-reduced ejection fraction.
We mentioned above that benefits in HFpEF are similar to those seen in HFrEF.
If 100 people with HFpEF take an SGLT2i for 2 years (gpevidence.org, accessed October 2025):
- 3.1 avoid hospitalisation with heart failure (NNT 32).
- 0.9 avoid cardiovascular death (NNT 188).
Supporting evidence for MRAs in HFpEF
Choice of drug
NICE does not recommend a particular MRA by name in its guidance (NICE 2025, NG106), but it does restrict the use of finerenone (a non-steroidal MRA) to the treatment of CKD in those with type 2 diabetes (NICE 2023, TA877). The two remaining options are spironolactone or eplerenone. Note that eplerenone is unlicensed for HFpEF, and spironolactone is licensed for moderate to severe heart failure (type not specified) or to treat oedema in heart failure. Thus, we may be prescribing ‘off-label’ for some of our patients.
Finerenone in European guidelines
Finerenone is recommended in the 2023 update to the 2021 European Society of Cardiology heart failure guideline to reduce the risk of hospitalisation with heart failure in those with CKD and type 2 diabetes (EHJ 2023;44:3627).
Evidence
MRAs reduce hospitalisation with heart failure and improve all-cause mortality and cardiovascular deaths in HFpEF, albeit with a risk of hyperkalaemia. Key trials include TOPCAT and FINEARTS-HF, which looked at spironolactone and finerenone respectively. Initially, spironolactone was thought to be ineffective in HFpEF, but subsequent review of the data (after removal of misdiagnosed patients) demonstrated benefit (TOPCAT NEJM 2014;370:1383 and subsequent review in Circulation 2015;131:34).
The FINEARTS-HF trial was an international, double-blind RCT randomising patients to either finerenone or placebo, in addition to usual therapy. 6000 patients with preserved or mildly-reduced ejection fraction heart failure were randomised; median follow-up was 32 months and the endpoint was a composite of ‘heart failure events’ and death from cardiovascular causes. Finerenone resulted in a ‘significantly lower event rate’ in the composite endpoint, but, if we take ‘cardiovascular death’ in isolation, the result is non-significant (hazard ratio 0.94; 95% CI 0.78–1.11) (NEJM 2024;391:1475). The accompanying editorial postulates that failure to reach CV death significance is most likely due to the trial being underpowered because the rate of CV death in those with HFpEF is significantly lower than those with HFrEF (NEJM 2024;391:1540).
No head-to-head trials compare spironolactone with finerenone.
Medication in heart failure management: starting and monitoring
Cardiac rehabilitation
NICE says that a personalised, exercise-based cardiac rehabilitation programme should be offered to all with heart failure. It should be tailored to the individual and be provided in a way that is accessible to the patient (home, community or hospital). It should include educational and psychological components, and may be incorporated within an existing rehabilitation programme. The MDT should refer patients to cardiac rehabilitation.
Chronic heart failure reviews
NICE suggests that review takes place at least every 6 months for those with stable disease, but more frequently (days to every 2 weeks) if the clinical condition or medication changes (NICE 2025, NG106). Review should cover:
- Clinical assessment of functional capacity.
- Fluid status.
- Cardiac rhythm (by checking the pulse).
- Cognitive status.
- Nutritional status.
- Medication review.
- Renal function assessment.
- Iron status and haemoglobin measurement.
(This list is a minimum and doesn’t include monitoring comorbidities.)
Who should do the review? NICE tells us that we need to review all patients with heart failure in primary care at least every 6 months. It does not specify that the list (above) must be done by primary care because some patients will have had some of this done by the MDT. This guidance from NICE allows us to take a pragmatic approach and do anything that’s missing or overdue.
Note that NICE does not recommend monitoring NT-proBNP in the community, but this may be used in specialist settings to optimise treatment.
The NYHA functional assessment
NICE doesn’t mention the NYHA classification in the ‘clinical review’ section of the heart failure guideline, only the requirement to record functional capacity. However, NICE does specify that NYHA should be used in its IND195 guidance. It is also required for QoF (2025–26) (NICE 2019, IND195).
| Category | Description (Symptoms may be breathlessness, fatigue, palpitation or chest pain) |
| NYHA I | No limitation of physical activity. |
| NYHA II | Slight limitation of physical activity (comfortable at rest, but ordinary activity causes symptoms). |
| NYHA III |
Marked limitation of physical activity (comfortable at rest, but minimal activity causes symptoms).
|
| NYHA IV | Symptoms at rest. |
| (Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels 9th Ed. Little, Brown & Co. Boston, Mass 1994:253). | |
Palliative care
NICE makes the following recommendations (NICE 2025, NG106):
- Involve the MDT if a person is worsening despite optimal specialist treatment, and discuss palliative care needs.
- Offer people with heart failure and their family or carers access to palliative care professionals.
- Follow NICE’s guidance on the care of dying adults.
- Do not use prognostic risk tools to decide whether to involve palliative care services.
- Do not offer long-term oxygen for advanced heart failure.
A BMJ article on palliative care in heart failure suggests that other considerations may include (BMJ 2016;352:i1010):
- Deactivation of implantable defibrillators.
- Good palliative care. At the end stage of heart failure, the disease often affects quality of life more than other diseases.
- Polypharmacy and frailty. Comorbidity is very common, polypharmacy is the norm and patients are often frail.
- Prognostic uncertainty. One of the challenges is the uncertain trajectory of the disease. Whereas people with cancer tend to slowly deteriorate, those with heart failure tend to have periods of stability with sudden exacerbations, and, during these exacerbations, it is difficult to predict whether this dip is recoverable or a terminal event. This is challenging for patients, carers and professionals! One study showed that patients tend to overestimate their life expectancy by over 40%, suggesting that they may not be ready to discuss end-of-life issues when those conversations are perhaps needed.
- Clear communication. Good communication with the other professionals involved is important; if primary care is having end-of-life discussions while the cardiologist is offering some kind of pump assist device or implanted defibrillator, the patient may well be confused – although doing both may be entirely reasonable!
The BMJ article raised a number of questions about how we provide care for people with heart failure:
- Have you given your heart failure patients the opportunity to ask/talk about their prognosis?
- Have you talked about symptom control, symptom by symptom?
- Have you talked about non-drug options too? We know about opioids and benzodiazepines for breathlessness, but what about a fan to blow air across the face?
- Have you given them the opportunity to talk about end-of-life issues (advance directives, DNAR, preferred place of death)?
- Have you looked for and treated depression and anxiety?
Dilemmas in chronic heart failure
Lifestyle dilemmas
Is exercise safe in heart failure?
Regular exercise has been shown to improve quality of life and exercise capacity. Formal activity programmes or cardiac rehabilitation have proven to be beneficial. Reduced activity can lead to deconditioning, further exacerbating symptoms (BMJ 2024;384:e077057). HF-ACTION demonstrated some reduction in hospitalisations with heart failure in those with improved exercise capacity (JAMA 2009;301:1439).
Does low-sodium diet improve outcomes?
No!
A Canadian RCT looked at whether restricting dietary sodium (<1.5g/day) affected risk of admission to hospital with heart failure, all-cause mortality or ability to complete a 6-minute walking test (Lancet 2022; 399:1391):
- No significant improvement in clinical outcomes from restricting dietary sodium.
- Slight improvements in patient-reported quality of life and clinician-assessed NHYA functional class.
NICE heart failure guidance does not recommend routinely restricting salt intake for people with heart failure (NICE 2025, NG106).
What about salt substitutes?
No!
NICE does not recommend potassium-based salt substitutes in chronic heart failure (NICE 2025, NG106). This is due to risk of hyperkalaemia, particularly in those taking ACE/ARBs and MRAs.
Can I drive?
DVLA guidance changes frequently and it’s important that we give up-to-date information so we signpost here to the DVLA guidance. In general, for less severe heart failure, it is likely that group 1 (car) driving will be permitted. It is likely that group 2 (bus and lorry) drivers will at least need to inform the DVLA, even for mild and stable disease.
Is air travel permitted?
Usually.
NICE advises that “air travel will be possible for most people with heart failure, depending on their clinical condition at the time of travel” (NICE 2025, NG106). If in doubt, we suggest liaising with the MDT.
Treatment dilemmas
Do loop diuretics have a long-term mortality benefit?
No. Loop diuretics are used to help symptoms associated with fluid overload. Up- or down-titrate according to need. Use the lowest dose required (NICE 2025, NG106). The aim of diuretics is to reduce hypervolaemia. Once euvolaemia is achieved, the dose can be reduced to the lowest effective dose or potentially stopped altogether (Aust Prescr 2022;45:200). If discontinued, 'it would be pragmatic to safety-net, e.g. symptoms to watch for or, in some patients, daily weight (which is mentioned in the ESC 2021 guideline but not covered by NICE).
GLP1-mimetics for heart failure?
These agents are not (yet) recommended in any heart failure guideline. Here, we summarise the emerging evidence, which is mainly industry-sponsored.
HFrEF:
In summary, the evidence does not demonstrate benefit of GLP1-mimetics in HFrEF.
- FIGHT RCT: 300 non-diabetic people admitted acutely with HFrEF. Does liraglutide improve clinical stability? No (JAMA 2016;316:500).
- LIVE RCT: 240 patients (with and without T2DM) with stable HFrEF randomised to liraglutide or placebo. No effect on ventricular systolic function, but more serious cardiac adverse events occurred (Eur J Heart Fail. 2017;19:69).
We were unable to find any dedicated trials in HFrEF looking at semaglutide or tirzepatide.
HFpEF:
In summary, there is some evidence of benefit for GLP1-mimetics in obesity-related HFpEF.
- STEP-HF trial: 500 people with HFpEF and a BMI ≥30 (without diabetes). The trial found that semaglutide improved symptoms and physical limitations over a 12-month period (NEJM 2023;389:1069).
- Improvement in the composite endpoint of ‘cardiovascular death or worsening heart failure’ relied on the ‘worsening heart failure’ group. Cardiovascular death reduction in isolation was non-significant (Lancet 2024;404:949).
- SELECT trial (subset analysis): an RCT of semaglutide in over 41 countries (17 600 patients). The trial asked if semaglutide was helpful for heart failure outcomes in patients with atherosclerotic heart disease AND overweight/obesity (it included patients with and without heart failure at enrolment). It found that semaglutide reduced all-cause mortality, cardiovascular death, cardiovascular events and heart failure endpoints compared with placebo. This effect was demonstrated over ALL types of heart failure (Lancet 2024;404:773).
- SUMMIT: an RCT compared weekly tirzepatide with placebo in 731 patients with heart failure with preserved ejection fraction (EF ≥50%) and obesity (BMI ≥30) (NEJM 2025;392:427). Median follow-up was 2 years. It found significant improvement in the composite primary endpoint of ‘reduced risk of CV death or worsening HF events’ (15.3% reduced to 9.9%), mainly due to the reduction in HF events:
- Worsening HF events fell from 14.2% on placebo to 8.0% with tirzepatide.
- Interestingly, there were more CV deaths in those on tirzepatide than placebo (note that the absolute numbers were small).
Combining ACEi and ARB
This is not something for primary care to initiate!
There are some theoretical benefits, and it is only occasionally seen in clinical practice. It is not recommended in the NICE chronic heart failure guideline (NICE 2025, NG106).
The MHRA issued a warning about using an ACE inhibitor with an ARB. The risks are hyperkalaemia, hypotension and impaired renal function (MHRA, June 2014). However, for heart failure, it concluded:
- In carefully selected people, the benefits may outweigh the risks.
- In this situation, an MRA should NOT be used.
- This combination should not be used in those with diabetic nephropathy (already prone to developing hyperkalaemia).
Are ARBs as good as ACEi drugs?
ARBs lack the weight of evidence seen with ACE inhibitors. ELITE II failed to show superiority of ARB over ACEi. ACEi drugs remain first choice due to weight of evidence (DTB 2025;63:133).
Beta-blockers: bradycardia
NICE tells us (NICE 2025, NG106):
- Carry out an ECG before starting a beta-blocker for heart failure.
- Do not start a beta-blocker if the patient has bradycardia (HR <50/min) or second or third-degree heart block (unless they have a pacemaker).
- For people on a beta-blocker who have symptoms and bradycardia, repeat the12-lead ECG after each dose increase to detect new arrhythmias or conduction abnormalities (NICE does not say that we should stop or reduce therapy!).
- No suggested action for asymptomatic people with bradycardia.
The NICE guidance left us a little puzzled. Should we really do nothing if we discover bradycardia in an asymptomatic person treated with a beta-blocker for heart failure? We performed a literature search.
- The DTB tells us that after starting a beta-blocker, subsequent asymptomatic hypotension or bradycardia does not warrant dose reduction unless there is other evidence of hypoperfusion (DTB 2025;63:133).
- The BNF lists bradycardia as a caution rather than contraindication.
- The ESC guidance (ESC, 2021, supplementary table 3), like NICE, does not make any suggestion for down-titration in asymptomatic people with bradycardia. No lower heart rate limit is mentioned.
It seems that the message is: in heart failure, unless there are symptoms indicative of an adverse effect, we continue the beta-blocker. At Red Whale, our bravery has a limit. We would probably use our clinical judgement and likely repeat an ECG and/or seek advice from cardiology.
Statins for heart failure
Statins do not confer specific benefit in heart failure (ESC guidance European Heart Journal 2021;42:3599).
Statins are not mentioned in the NICE chronic heart failure guideline (NICE 2025, NG106).
Ivabradine
NICE reserves this for specialist use (NICE 2025, NG106) (NICE 2012, TA267).
Ivabradine is an inhibitor of the sinoatrial node and therefore slows heart rate.
Beta-blockers also slow heart rate, but have a detrimental effect on myocardial contractility. Using ivabradine could provide some of the benefits of beta-blockers without the downsides. It can also be used for angina.
Metolazone
Metolazone is not specifically mentioned in the NICE chronic heart failure guideline. It may be a specialist-only drug in your locality. An MHRA Drug Safety Update included prescribing information for metolazone, one of our less commonly used thiazide diuretics (Drug Safety Update 2023;16:1).
- There is now a licensed product available in the UK (previously, all versions were unlicensed).
- The licensed drug has twice the bioavailability of the unlicensed version, meaning that doses of the new licensed drug should be half the equivalent unlicensed version.
MHRA advice:
- The decision to transfer a patient from one formulation to another should be made by a specialist.
- Clinical systems should record whether the patient is on the licensed or unlicensed version, and this information should be handed over at every transfer of care.
- Patients starting metolazone should be prescribed the licensed version.
Which drugs should we AVOID in heart failure?
The DTB lists the following (DTB 2025;63:133):
- NSAIDs (worsen congestion).
- Thiazolidinediones (which we know as the ‘glitazones’!) (worsen congestion).
- Doxazosin (risk of fluid retention and reflex tachycardia).
- Non-dihydropyridine calcium channel blockers (e.g. verapamil) (these impair myocardial contraction).
- Class I antiarrhythmic drugs (e.g. quinidine, flecainide) (we don’t tend to prescribe these in primary care).
Cardiac resynchronisation
This involves pacing both ventricles. A standard pacemaker is either single chamber (right ventricle) or dual chamber (right atrium and right ventricle). In resynchronisation, leads pace the right atrium, the right ventricle AND the left ventricle. Pacing both ventricles improves coordination of atria and ventricles to improve cardiac function. Evidence shows that it reduces hospitalisation and mortality and is cost-effective. Patients of all ages benefit so this can be considered even in those who are quite elderly (BMJ 2009;338:b1265).
Evidence is now emerging that suggests only those with left bundle branch block are likely to get benefit, and that there are benefits (reduced mortality) even in those with mild heart failure (NEJM 2014;370:1694). However, NICE’s guidance currently restricts use to those with more severe disease (NICE 2014, TA314).
Clearly, we won’t be making this decision, but we probably will see increasing numbers of our patients with heart failure being fitted with a pacemaker for this reason.
Comorbidity dilemmas
Urinary incontinence
Studies suggest that 35–50% of people with heart failure have urinary incontinence (BMJ 2021;374:n1593).
It is likely to be multifactorial: diuretics, perhaps an ACE inhibitor-induced cough, frailty.
What is more, the incontinence may lead to reduced adherence to therapy and worsening disease control.
How often do we ask our patients about this?
It’s not an easy problem to solve, but changing the time at which diuretics are taken can reduce night-time issues, and pelvic floor exercises and bladder training may help. And it’s important to know what medication is ACTUALLY being taken because it may affect decisions we make with regard to other drugs.
Ankle swelling in those with known heart failure
If a patient with known heart failure develops new or worsening ankle swelling, it is important to consider the differential diagnoses (BMJ 2020;369:m2099):
- Decompensated heart failure.
- DVT.
- Cellulitis.
- CKD.
- Chronic liver disease.
- Chronic venous insufficiency.
- Lymphoedema.
- Hypoalbuminaemia.
- Drugs: calcium channel blockers, alpha-blockers, hydralazine, testosterone.
Causes of decompensated heart failure include:
- Non-adherence to medication or under-dosing with diuretics.
- Excessive fluid intake.
- AKI.
- Significant new arrhythmia.
- Acute coronary syndrome.
- Infection.
- Medication: NSAIDs, steroids/negative inotropes/chemotherapy.
- Hypertensive emergency.
Many of you will have been taught that furosemide has an ‘all or nothing’ effect: as you increase the dose, you flick a switch and it starts to work; below this dose, it does not. However, this is apparently not the case – and we were all taught this because the original researchers misinterpreted the dose response curves (easy to do, I hear!). And thank you to the Midlands and East Medicines Advice Service for explaining this to us so clearly! (Cardiovascular Pharmacotherapy 2019;5:246)
|
Chronic heart failure
|
|
|
Do your patients receive 6-monthly heart failure reviews? Is renal function and potassium monitoring taking place regularly? Have you talked about end-of-life planning with your patients? Do you have access to cardiac rehabilitation for heart failure patients? |
|
|
Useful resources: Websites (all resources are hyperlinked for ease of use in Red Whale Knowledge) |
This information is for use by clinicians for individual educational purposes, and should be used only within the context of the scope of your personal practice. It should not be shared or used for commercial purposes. If you wish to use our content for group or commercial purposes, you must contact us at sales@red-whale.co.uk to discuss licensing, otherwise you may be infringing our intellectual property rights.
Although we make reasonable efforts to update and check the information in our content is accurate at the date of publication or presentation, we make no representations, warranties or guarantees, whether express or implied, that the information in our products is accurate, complete or up to date.
This content is, of necessity, of a brief and general nature, and this should not replace your own good clinical judgment or be regarded as a substitute for taking professional advice in appropriate circumstances. In particular, check drug doses, side effects and interactions with the British National Formulary. Save insofar as any such liability cannot be excluded at law, we do not accept any liability for loss of any type caused by reliance on the information in these pages.
Here is the link to our terms of use.