
This Pearl is provided as free content. Here is the link to our terms of use
Headaches (non-migraine): diagnosis and management
Headaches (non-migraine): diagnosis and management
I’d been treating her for migraines for a while. She kept coming back, saying, “My migraines are no better”, and I kept stepping up both her relievers and preventers. And then, one day, she came to see me when she actually had a migraine. She was clutching her head and pacing up and down my room. Suddenly, I realised that the ‘migraines’ I had been treating for months were not actually migraines but cluster headaches! When I got the treatment right, she improved considerably. Looking back, it was all there in the history….
This article was last updated in December 2023.
This article focuses on:
- Headache red flags.
- Tension headache.
- Cluster headache.
- Cervicogenic headache.
- Medication-overuse headache.
It is based on the NICE guidance on headaches in over-12s (NICE 2012, CG150) and the SIGN guidance on pharmacological management of migraine, which covers medication-overuse headache (SIGN 155, 2023).
For information on migraine, please see the article Migraine in adults. For information on idiopathic intracranial hypertension, see article: Headache and raised intracranial pressure. For information on subarachnoid haemorrhage, see article: Thunderclap headache and subarachnoid haemorrhage.
There is an example of a headache diary in a separate online article, Headaches: weekly headache diary.
Headache: GEMS
Please follow the link for a PDF version of the GEMS for download/printing: Headache: GEMS
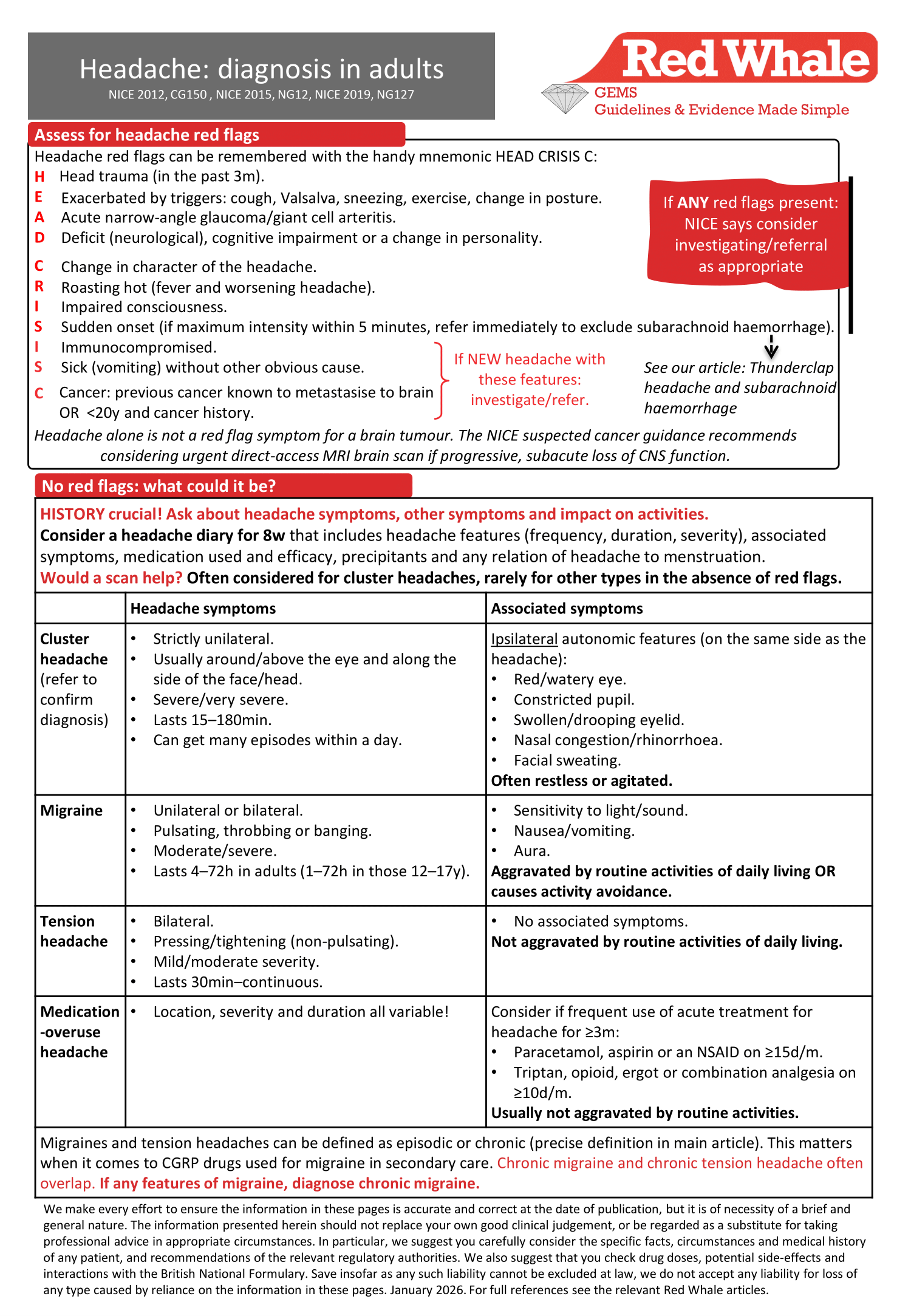
(NICE 2012, CG150 , NICE 2015, NG12, NICE 2019, NG127)
Tension headaches
Tension headaches can be defined as episodic or chronic (NICE 2012, CG150):
- Episodic: headache on <15d/month.
- Chronic: headache on ≥15d/month for >3m.
Management of tension headaches in non-pregnant adults
| Acute treatment | Prophylaxis |
|
|
Cluster headaches
Refer for confirmation of diagnosis: may need imaging.
Cluster headaches can be defined as episodic or chronic (NICE 2012, CG150):
- Episodic: occur between once every 2 days to up to 8 times/d AND pain free for >1m.
- Chronic: occur between once every 2 days to up to 8 times/d AND not managing 31 days without symptoms within the span of a year
Management of cluster headaches in non-pregnant adults (NICE 2012, CG150):
| Acute treatment | Prophylaxis |
|
|
What about steroids for cluster headache?
NICE does not mention the use of steroids for cluster headache (NICE 2012, CG150).
A Lancet comment on the topic pointed out that although oral corticosteroids have been used for over 40 years for cluster headaches, there is a lack of high-quality evidence for their use (Lancet 2021;20(1):19). A secondary care decision!
GammaCore for cluster headaches in secondary care
This is a non-invasive vagus nerve stimulator used to treat and prevent cluster headaches. It will be initiated by a specialist and considered in those who do not respond to standard treatment. What do we need to know about it? (NICE 2019, MTG46, NICE 2018, MIB 162):
- GammaCore is a non-invasive vagus nerve stimulator for treatment of cluster headaches:
- It is applied to the neck surface and modifies pain signals by stimulating the vagus nerve in the neck.
- The patient controls a handheld device which delivers a small electric current. It is generally well tolerated.
- It should be used regularly throughout the day to prevent cluster headache attacks, and acutely to reduce pain during an attack.
- It appears to work well in some people, but not all (works in 25–50%). It will only be continued in people who find it effective after the first 3m of treatment.
- It is contraindicated in those with an active implantable medical device, heart disease or during pregnancy, and cannot be used in children.
Complementary and integrative medicine for headache
A BMJ State-of-the-Art review considered the evidence for complementary and integrative medicine in the management of headache (BMJ 2017;357:j1805). The review assessed meta-analyses, systematic reviews and RCTs; however, the majority of the evidence was of low to moderate quality. It found:
- Acupuncture, massage, yoga, biofeedback and meditation helped tension headache.
- These interventions have not been assessed in the management of cluster headache.
What is cervicogenic headache?
Cervicogenic headache is a headache due to an underlying neck problem. To diagnose cervicogenic headache, there needs to be (International Headache Society, 2021):
- A neck problem (or a lesion in the cervical spine/surrounding tissues seen on imaging) which can cause a headache AND at least 2 of the following:
- The onset of the headache is related to the onset of the neck problem/lesion.
- The headache improves/resolves with improvement/resolution of neck problem/lesion.
- Range of movement of neck is reduced and headache worsens with certain neck movements.
- Headache resolves with a nerve block of a cervical structure.
Cervicogenic headache, migraine and tension headache all have crossover symptoms, introducing uncertainty and making a positive diagnosis of cervicogenic headache more challenging. We may have to look to other features to guide us towards or away from each diagnosis; there’s no reliable single test.
For instance, reduced range of neck movement and reduced neck flexion strength have been proposed as a way of differentiating cervicogenic headache from migraine (BMC Musculoskeletal Disorders 2021;22:755). However, stiff necks are really common so it’s no surprise that the specificity figures aren’t great (70–90%). If you’re in doubt, a physiotherapist could assess the likelihood of posterior headache with nausea or photophobia being neck-related (likely faster to access than neurology!). In forming an opinion, the physio may manage any neck stiffness (incidental or otherwise), thus helping your patient in the process!
Medication-overuse headaches
What is medication-overuse headache?
(SIGN 155, 2023, NICE 2012, CG150)
- It is a headache on ≥15d/m while taking regular acute headache treatment for >3m. Regular acute headache treatment is:
- ≥15d/month taking simple analgesia (aspirin, ibuprofen, paracetamol).
- ≥10d/month taking triptans, combination analgesia, opioids or ergots.
- It only occurs if acute analgesic medication is being used to treat an underlying headache disorder, not if using them for another painful condition, e.g. arthritis (DTB 2010;48:2).
- There is an increased risk if acute headache treatment used frequently (>2d/w).
- Risk factors include frequent headache, frequent acute medication, pain from another cause, mental health condition.
- Medication-overuse headache accounts for 1% of headaches worldwide, and 80% are secondary to acute drug treatment for migraine.
However, frequent headache in those taking frequent acute medication is not always medication-overuse headache. It may be poorly-controlled migraine (SIGN 155, 2023)!
The self-perpetuating cycle of medication-overuse headache:
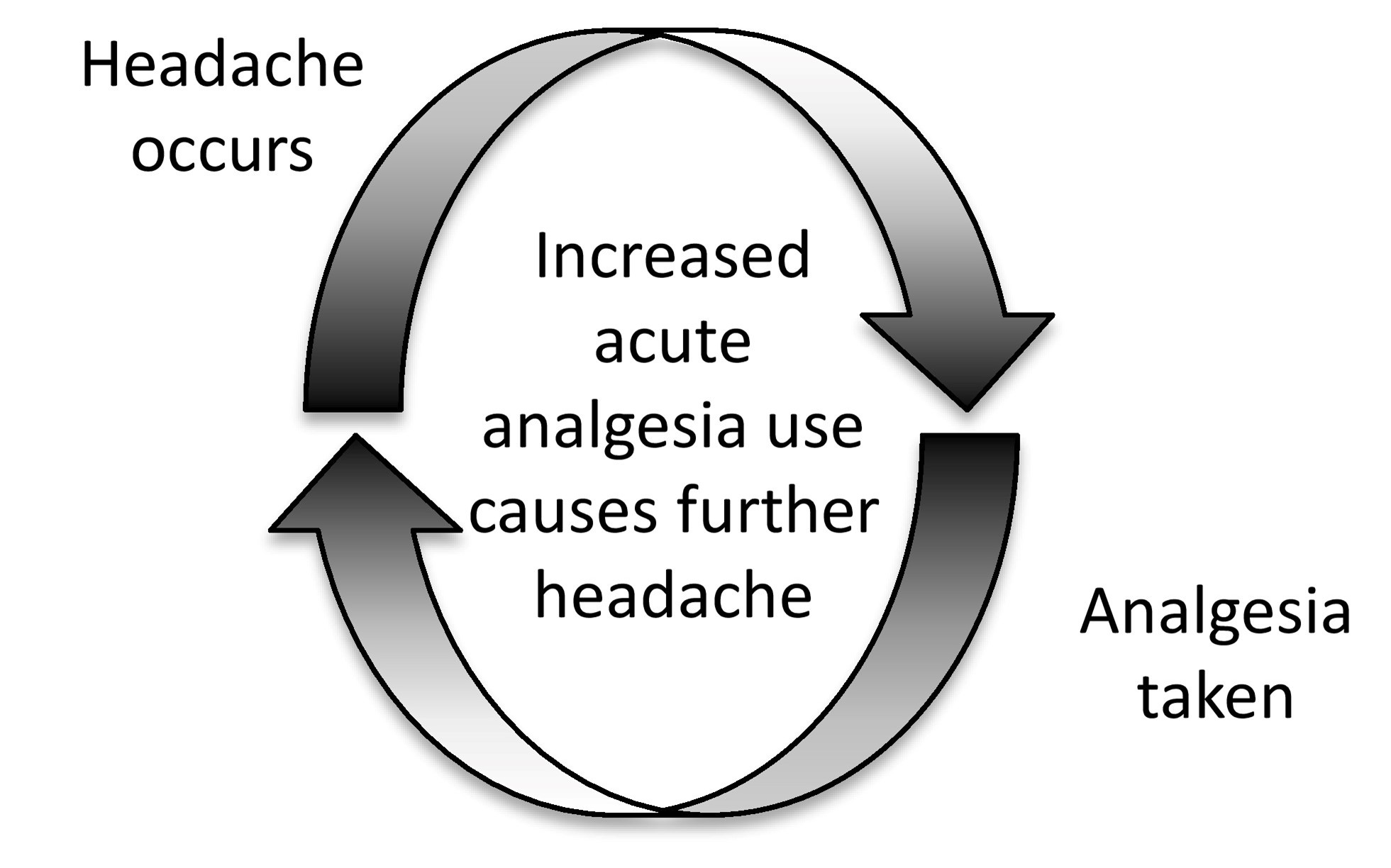%20-%20diagnosis%20and%20management%20-%20medication-overuse%20headache.jpg?version=1)
Treatment of medication-overuse headache
Prevention is better than cure! Discuss the risk of medication-overuse headache with anyone taking regular acute medication for a headache disorder (SIGN 155, 2023).
Stopping overused medication can reduce headache frequency and intensity; however, headache will often worsen transiently before improving (SIGN 155, 2023, NICE 2012, CG150).
SIGN and NICE have slightly different approaches to management (SIGN 155, 2023, NICE 2012, CG150):
Management of medication-overuse headache | |
| NICE (NICE 2012, CG150) | SIGN (SIGN 155, 2023) |
|
Either:
For ALL options, if taking opioids, consider withdrawal gradually (not abruptly). |
Medication-overuse headache troubleshooting
How quickly should the headaches improve on stopping the drugs (DTB 2010;48:2)?
- For simple analgesia: 2–3w.
- For opioids: 2–4w.
- For triptans: 7–10d.
Managing withdrawal symptoms (DTB 2010;48:2):
- Nausea and vomiting are common, but antiemetics can be used.
Failure of therapy (withdrawal of drugs fails to reduce headaches) more likely if (DTB 2010;48:2):
- People have been on therapy for a long time.
- People are on drugs other than triptans (triptan medication-overuse headaches have a relatively good prognosis).
- Underlying headache is a tension headache.
- High levels of self-reported bodily pain or poor sleep.
Once successfully off the causative drug, make sure the patient knows to avoid using it more than twice a week or they risk the medication-overuse headaches recurring. (Relapse is common: 30% by 6m, 40% at 1y, 45% at 4y.)
|
Headaches (non-migraine): diagnosis and treatment
For tension headaches:
For cluster headaches:
Medication-overuse headaches:
|
|
| Audit your last 10 consultations of patients with longstanding headache: could they have a medication-overuse headache? |
This information is for use by clinicians for individual educational purposes, and should be used only within the context of the scope of your personal practice. It should not be shared or used for commercial purposes. If you wish to use our content for group or commercial purposes, you must contact us at sales@red-whale.co.uk to discuss licensing, otherwise you may be infringing our intellectual property rights.
Although we make reasonable efforts to update and check the information in our content is accurate at the date of publication or presentation, we make no representations, warranties or guarantees, whether express or implied, that the information in our products is accurate, complete or up to date.
This content is, of necessity, of a brief and general nature, and this should not replace your own good clinical judgment or be regarded as a substitute for taking professional advice in appropriate circumstances. In particular, check drug doses, side effects and interactions with the British National Formulary. Save insofar as any such liability cannot be excluded at law, we do not accept any liability for loss of any type caused by reliance on the information in these pages.
Here is the link to our terms of use.