
This Pearl is provided as free content. Here is the link to our terms of use
Bias in healthcare
Everyone holds biases. These develop through lifelong exposure to social and cultural influences – including family, education and the media – which shape our attitudes and expectations over time. In healthcare, these biases can affect how clinicians perceive, communicate with and make decisions about patients, even when we consciously intend to treat everyone fairly.
Although bias cannot be completely eliminated, greater self-awareness and reflection can help reduce its influence. Recognising our own biases – and taking deliberate steps to ensure they do not shape our professional behaviour – is an important part of providing fair, effective healthcare.
This article explores how bias can affect healthcare, and what we can do to minimise its impact in practice.
We recognise that language is important when discussing bias. In this article, we have used gender, ethnicity and disability terminology as used by the study authors when reporting specific papers, and have otherwise followed appropriate inclusive language guides (gov.uk - writing about ethnicity, gov.uk - inclusive language: words to use and avoid when writing about disability, NHS Digital Service Manual – sex, gender and sexuality).
This article was written in April 2026.
What is bias?
Bias refers to a systematic pattern of thinking or decision-making that unfairly favours certain groups, individuals or viewpoints. It often involves making judgements about another person based on characteristics that are not relevant to the situation, such as race or gender. Bias can be:
- Explicit: involving conscious and deliberate attitudes or behaviours.
- Unconscious (also known as implicit): operating outside conscious awareness.
Unconscious bias can influence how we perceive and respond to others across many aspects of identity and personal background, including race, gender, age, sexuality or LGBTQIA+ status, disability, socioeconomic background, weight and health conditions.
Some important related terms include:
- Stereotypes: overgeneralised or negative beliefs about members of a particular group – for example, assuming that poor people are lazy or that Black patients are less likely to follow medical advice.
- Prejudice: negative attitudes or feelings toward a person or group that are formed before any personal experience, with emotional, cognitive and behavioural components.
- Intersectionality: the experience of belonging to more than one marginalised or disadvantaged group, leading to overlapping or compounded forms of bias (for example, a Black, disabled woman).
(Int J Environ Res Public Health 2023;20:6569)
Why does unconscious bias arise?
Unconscious bias arises when judgements or decisions are shaped by prior experiences and assumptions, without our awareness.
Human thinking involves two interacting systems (Future Health J 2021;8:40):
- Fast thinking is automatic and intuitive, using mental shortcuts to categorise people and situations based on stereotyped patterns learned from our own experiences and from those around us. It is efficient and supports rapid decisions and emotional responses. However, because it operates largely outside conscious awareness, it can create blind spots and is more vulnerable to unconscious bias. In healthcare, this may contribute to differences in how patients are perceived, understood or treated.
- Slow thinking is deliberate and analytical, used for complex reasoning and unfamiliar problems. It allows more careful reflection, but requires time and mental effort, which may limit its use in busy or time-pressured settings.
Clinical work typically involves both systems. For example, a clinician may use analytical reasoning to decide which medication to prescribe, while relying on well-practised automatic skills when performing a procedure.
Both systems are essential, but recognising when fast thinking may be shaping decisions without awareness is key to reducing the impact of bias.
Cultural context and influences
Biases develop gradually through repeated exposure to cultural messages, social norms and stereotypes that associate particular groups with certain traits or behaviours (The Royal Society 2015). Over time, these associations can become embedded in our thinking, often without conscious awareness.
People tend to feel more comfortable with individuals who appear familiar or similar to themselves, while those who seem different may be approached with greater caution or uncertainty. These subtle preferences can influence how clinicians interpret competence, motivation or trustworthiness, even when there is no conscious intention to treat people differently.
Situational and system factors
Working conditions can also increase the likelihood that unconscious bias influences decision-making. Clinical practice often involves time pressure, high patient volume, interruptions and uncertainty. Factors such as fatigue, stress, cognitive overload and decision fatigue can all reduce the capacity for analytical (slow) thinking and increase the risk of unconscious bias (BMJ Quality & Safety 2013;22:ii58).
This is a reminder that bias is not just about individual attitudes, but is also influenced by the systems and environments in which healthcare is delivered – including workload pressures, organisational culture and structure. Addressing these wider factors may be an important part of reducing bias. At the same time, in day-to-day practice, recognising these influences can help us question our first impressions. A brief pause to step back and reconsider can bring a broader and more balanced perspective.
Other types of bias
Unconscious bias is one of many forms of cognitive bias that can influence judgement and decision-making. In clinical practice, these biases can affect consultations, diagnostic reasoning, treatment decisions and the interpretation of results or evidence. These influences may also contribute to wider inequalities within healthcare systems, including disparities in leadership, career progression and pay. Cognitive biases have also been linked to diagnostic errors, inappropriate management decisions and missed opportunities for care (Future Health J 2021;8:40).
The table below summarises some common examples relevant to everyday clinical practice:
| Type of bias | What does this involve? | Example in healthcare |
| Anchoring | Relying too heavily on an initial impression or piece of information, and failing to adjust when new evidence emerges. | Attributing chest pain to anxiety because the patient has previously presented with panic attacks, without reconsidering cardiac causes. |
| Availability bias | Judging likelihood based on how easily examples come to mind, often influenced by recent or memorable cases. | Overestimating the likelihood of a rare condition because of a recent experience where it was missed. |
| Confirmation bias | Seeking or interpreting evidence that supports an existing diagnosis while overlooking conflicting information. | Continuing to treat for infection while discounting test results or symptoms that suggest another diagnosis. |
| Framing effect | Being influenced by how information is presented or labelled, rather than by the underlying facts. | Interpreting symptoms differently depending on whether the referral describes the patient as ‘anxious’ or as having ‘chest pain of uncertain cause’. |
| Commission bias | A tendency to favour intervention or action, rather than watchful waiting, even when it may not be necessary. | Ordering imaging or starting medication ‘just in case’, despite low clinical suspicion. |
| Omission bias | Avoiding action because of concern about causing harm, even when inaction may carry greater risk; may be linked to risk aversion. | Delaying escalation of treatment because of fear of side-effects, despite clinical deterioration. |
| Overconfidence bias | Overestimating one’s knowledge or judgement, leading to decisions based on limited information. | A trainee being over-certain about a diagnosis made over the phone, without sufficient information or examination. |
| Hindsight bias | Believing, after an outcome, that it should have been obvious, distorting reflection and learning. | Self-blame after a missed diagnosis, assuming that the warning signs were clear at the time. |
| (BJA Educ 2021;21:420, BMC Med Inform Decis Mak 2016;16:138) | ||
These examples of cognitive bias are an important reminder of how easily our thinking and decision-making can be influenced in subtle ways, often outside our immediate awareness. These processes are a normal part of human decision-making, and the aim is not to eliminate them but to recognise that they exist. Keeping in mind that our decisions may be influenced by assumptions we do not immediately notice may sometimes prompt a brief pause to look again and consider whether another interpretation might be possible.
Bias and healthcare
A 2025 BMJ Analysis argues strongly that racism and sexism remain deeply embedded within the NHS, affecting both patient outcomes and staff experiences (BMJ 2025:390:r1334). Although the NHS is founded on equitable care, discrimination linked to protected characteristics, including race, sex, gender identity, disability, age and religion, continues to affect access to care, experiences of services and overall health outcomes.
These inequities contribute to higher rates of illness, poorer experiences of healthcare and increased mortality for some groups. They also carry substantial economic costs through lost productivity, increased welfare spending and additional healthcare expenditure. However, the report argues that meaningful progress has been limited by a lack of political and institutional commitment. Addressing inequities requires broad action across leadership, research, regulation, workforce culture and clinical practice.
Bias in clinicians
Health professionals are not immune to bias. A systematic review found evidence of unconscious bias among physicians and nurses across a range of patient characteristics, including age, race or ethnicity, gender, socioeconomic status, mental illness, disability, body weight and substance use. Clinicians demonstrated implicit biases at levels similar to those seen in the general population, which may influence how patients are perceived and assessed (BMC Med Ethics 2017;18:19).
Clinicians’ own characteristics – including gender, training, professional culture and clinical experience – can all play a role. For example, physicians have been found to demonstrate greater bias toward patients with mental health problems than psychiatrists, possibly reflecting differences in training and clinical exposure (BMC Med Ethics 2017;18:19).
Importantly, implicit biases can operate alongside consciously-held values of fairness and equality. This means that even well-intentioned clinicians may respond in biased ways, particularly under conditions of time pressure, fatigue, uncertainty or high cognitive load. Self-reported attitudes are therefore not reliable indicators of bias (Int J Env Res Pub Health 2023;20:6569).
How bias affects patient–clinician communication
Unconscious bias can influence the quality of interactions between clinicians and patients, often through subtle behaviours such as tone of voice, eye contact, body language or conversational style (The Royal Society 2015).
A systematic review found that patients who consulted clinicians with higher levels of implicit racial bias were more likely to perceive interactions as less respectful, less warm and less patient-centred (BMC Med Ethics 2017;18:19). These experiences can reduce trust and willingness to engage with care. Individuals who have experienced discrimination may also understandably approach medical consultations with greater caution, which can affect communication and trust on both sides.
A US cross-sectional study looking at primary care clinician attitudes found that patients from racially and ethnically diverse backgrounds reported lower interpersonal quality of care and poorer communication compared with White patients (Am J Public Health 2012;102:979). Many clinicians also showed an unconscious tendency to associate White patients with being more cooperative or compliant than Black patients. When clinician bias was stronger, consultations tended to involve:
- Less patient-centred communication, with clinicians talking more than patients.
- Fewer signs of warmth or positive engagement.
- Lower levels of trust, with Black patients less likely to feel respected or confident in the clinician.
These patterns are consistent with wider research suggesting that Black patients may experience more narrowly biomedical consultations, with fewer opportunities to discuss psychosocial concerns. Because patient-centred communication supports trust and adherence, this may also contribute to poorer health outcomes.
Bias and decision-making
Bias can influence clinical assessment, decision-making and management. It may affect (BMC Med Ethics 2017;18:19):
- The questions clinicians ask.
- The tests they order.
- How symptoms are interpreted.
- Treatment recommendations.
These effects often occur outside conscious awareness. Bias can alter what is seen as typical, credible or serious, influencing whether symptoms are explored further or attributed to less concerning causes. It may also affect assumptions about adherence, risk or motivation.
Bias and health inequalities
Unconscious bias can contribute to health inequalities through its impact on clinical decision-making and the quality of interactions. Differences in communication, trust and patient engagement, which are central to effective care, can affect health outcomes and future help-seeking behaviour (BMC Med Ethics 2017;18:19).
Bias may also appear as stereotypes that influence clinical judgement. Examples include (Future Health J 2021;8:40):
- Negative assumptions about non-White patients influencing treatment decisions and resulting in poorer outcomes.
- Weight bias, where obesity is attributed primarily to personal responsibility rather than complex contributing factors.
- Gender bias in the assessment of myocardial infarction, where women’s symptoms may be less likely to be recognised as cardiac in origin.
Ethnicity and race
People from Black, Asian and other minority ethnic groups experience poorer health outcomes in a range of areas associated with social inequality, discrimination and negative experiences within health systems. Examples include (BMJ 2025:390:r1334):
- Higher COVID-19 morbidity and mortality.
- Worse maternal and infant outcomes.
- Higher rates of mental illness and detention under the Mental Health Act.
- Lower likelihood of accessing early treatment through community pathways.
We discuss health inequalities related to ethnicity and race in more detail in our article, Racism and racial inequality.
Women’s health inequalities
The UK has a clear gender health gap, with women experiencing poorer health outcomes despite living longer than men. Although policy attention has increased – including the Women’s Health Strategy – it has largely focused on mortality, which is higher in men (LSE Public Policy Review 2025;3:1).
Women report higher levels of ill health, including chronic conditions, mental health problems and disability. They are also more likely to seek care and engage in preventive behaviours, but this does not translate into better outcomes. This points to differences in how symptoms are recognised and managed. Bias may contribute to symptoms being minimised or misattributed. In addition, much of the evidence base has historically been derived from male-dominated study populations. This has contributed to gaps in knowledge, differences in how conditions present being overlooked, and delays or inaccuracies in diagnosis and treatment for conditions affecting women.
Structural and social factors also play a role. Caregiving responsibilities, financial constraints and limited flexibility at work all make it harder for women – particularly in lower socioeconomic groups – to seek or follow-up care.
Other gender inequalities
LGBTQIA+ people also experience inequalities in both health outcomes and experiences of care. These are linked to discrimination, stigma and exclusion, which are associated with increased stress and higher rates of depressive symptoms. LGBTQIA+ individuals have higher rates of chronic illness, smoking, alcohol use and other factors associated with poorer physical health, as well as higher levels of mental health difficulties, including depression, stress and suicidality. This is particularly marked for transgender and gender-diverse individuals, and for some subgroups such as bisexual people (BMJ Open 2021;11:e049405).
However, gaps in healthcare provision, including limited clinician training and understanding of LGBTQIA+ identities, can further affect care. Within clinical encounters, bias may influence whether individuals feel able to disclose their identity, with implications for history taking, risk assessment and engagement with services. Assumptions about relationships, identity or risk may affect the questions asked and how information is interpreted, contributing to differences in how appropriate and safe care feels (Int J Environ Res Pub Health 2021;18:826).
Intersectionality
The impact of bias can be amplified when multiple aspects of identity intersect. Intersectionality describes how characteristics such as race, gender, disability or socioeconomic status combine to further compound disadvantage. For example, a Black woman living in poverty who is also disabled may experience substantially worse health outcomes than someone experiencing only one of these disadvantages (BMJ 2025:390:r1334).
This can affect how symptoms are interpreted and how seriously concerns are taken, contributing to differences in diagnosis and management. Some biases only emerge in combination, as shown in studies where clinical decisions vary depending on intersecting patient characteristics (BMC Med Ethics 2017;18:19).
Bias beyond clinical care
Bias can also affect policy and organisational structures. Institutional discrimination may arise through policies, systems and professional cultures that unintentionally disadvantage certain groups (BMJ 2025:390:r1334).
It may also influence research funding, interpretation of evidence and the development of clinical guidelines. These processes shape the evidence used in practice, meaning that bias at this level can contribute to differences in care at a population level (Future Health J 2021;8:40).
This highlights how bias can influence healthcare at many levels, from individual interactions to wider systems. It affects how people are listened to, understood and responded to, shaping trust, engagement and outcomes. These effects may be compounded when aspects of identity intersect. Recognising how bias operates in practice is an important step toward improving consistency and fairness in care.
Bias within workplaces
Bias can influence many aspects of working life, including how people are treated, supported and given opportunities within organisations. While it may sometimes be overt, it more often operates through routine processes and everyday interactions which affect access to opportunities, psychological safety and staff wellbeing.
Bias can influence multiple stages of employment, including:
- Recruitment: job descriptions, advertising methods, shortlisting decisions and interview processes.
- Career progression: access to development opportunities, promotions and leadership roles.
- Performance management: appraisals, feedback and opportunities for progression.
- Disciplinary processes: decisions about investigations, formal procedures and regulatory referrals.
- Workplace culture: day-to-day interactions, inclusion, respect and psychological safety.
Recruitment and career progression are particularly vulnerable to bias. Bias can influence how roles are defined, who is encouraged to apply, how candidates are assessed and how opportunities for advancement are allocated. Over time, small differences can accumulate and affect long-term career trajectories through unequal access to mentoring, development or leadership opportunities. Performance feedback and appraisal processes can also contribute, particularly where subjective expectations about competence or leadership potential may be shaped by bias.
Inequalities within the NHS workforce
Ethnic minority staff make up a substantial proportion of the NHS workforce, including clinicians, but often report poorer workplace experiences than White colleagues. This includes higher rates of bullying, harassment and discrimination. Many NHS staff have migrated to the UK to work in healthcare, but face additional pressures related to language, immigration status and cultural adaptation, which affect how supported and valued they feel (BMJ 2025:390:r1334).
These patterns are also reflected in career progression and organisational processes. Minority ethnic staff are under-represented in senior roles. White applicants are around 1.5 times more likely to be appointed from a shortlist, and minority ethnic staff are more likely to enter formal disciplinary procedures (BMJ Leader 2023;7:314).
Gender inequalities are also present. Women make up more than 75% of NHS staff, but experience higher rates of discrimination, sexual harassment and barriers to promotion (BMJ 2025:390:r1334). Female doctors are mistaken for nurses more often than male colleagues and may receive less favourable evaluations despite similar performance, while male clinicians are more likely to be introduced by their professional title (Future Health J 2021;8:40).
Bias also affects day-to-day workplace culture. Experiences such as incivility, exclusion or bullying may disproportionately affect marginalised groups, including minority ethnic, disabled and LGBTQIA+ staff. This can reduce psychological safety, making staff less likely to speak up, raise concerns or contribute fully within teams (BMJ Leader 2023;7:314).
Policies, procedures and training to promote fairness and reduce discrimination are important, but may have limited impact when used alone – increased awareness does not always lead to sustained changes in behaviour or decision-making.
Tackling bias
Recognising bias
The first step in addressing bias is recognising that it exists. Because many biases operate automatically and outside conscious awareness, people may believe they are acting objectively while underlying assumptions still influence their judgement. Acknowledging this can make it easier to approach decisions with curiosity and reflection.
Developing self-awareness can help bring these influences into view. This may involve reflecting on everyday interactions and decisions – for example, noticing whose views are heard most, or who is invited into discussions or offered opportunities. Asking whether the same judgement would be made if someone had a different background, gender or age can reveal assumptions that might otherwise go unnoticed. Colleagues can also help identify bias because it is often easier to recognise in others than in ourselves.
Self-awareness also involves noticing how emotions and personal experiences shape our perspective. Bias is more likely to influence decisions made under time pressure or cognitive overload, so pausing to question first impressions can sometimes support fairer and more thoughtful judgement.
However, awareness alone is unlikely to be sufficient. While unconscious bias training may increase understanding, evidence suggests that it does not consistently lead to sustained behavioural change when used in isolation (Future Health J 2021;8:40).
(NHS Midlands Leadership Academy – unconscious bias toolkit, The Royal Society, 2015, Int J Environ Res Public Health 2023;20:6569)
Challenging assumptions
Bias can lead to assumptions based on limited information or past experience. Reducing this risk involves focusing on relevant information and approaching each person as an individual. Practical approaches include:
- Asking open questions, discussing different perspectives and listening to understand, rather than to respond – recognising that others’ perspectives are shaped by their own experiences.
- Checking assumptions and ensuring decisions are based on evidence, rather than first impressions.
- Paying attention to verbal and non-verbal communication such as tone of voice, eye contact and body language to ensure interactions are respectful and inclusive.
Approaching differences with curiosity, rather than assumptions, can help challenge stereotypes and improve communication in both clinical and workplace settings.
(NHS Midlands Leadership Academy – unconscious bias toolkit)
Making thoughtful decisions
Bias is more likely to influence decisions made quickly or under pressure. Taking time to pause and reflect – particularly when making important clinical or organisational decisions – can help reduce this effect.
Using more structured approaches can also help slow automatic thinking. This might include reviewing the available evidence, considering alternative explanations and inviting input from colleagues. Hearing different perspectives and discussing decisions openly can help highlight blind spots and support more balanced judgement.
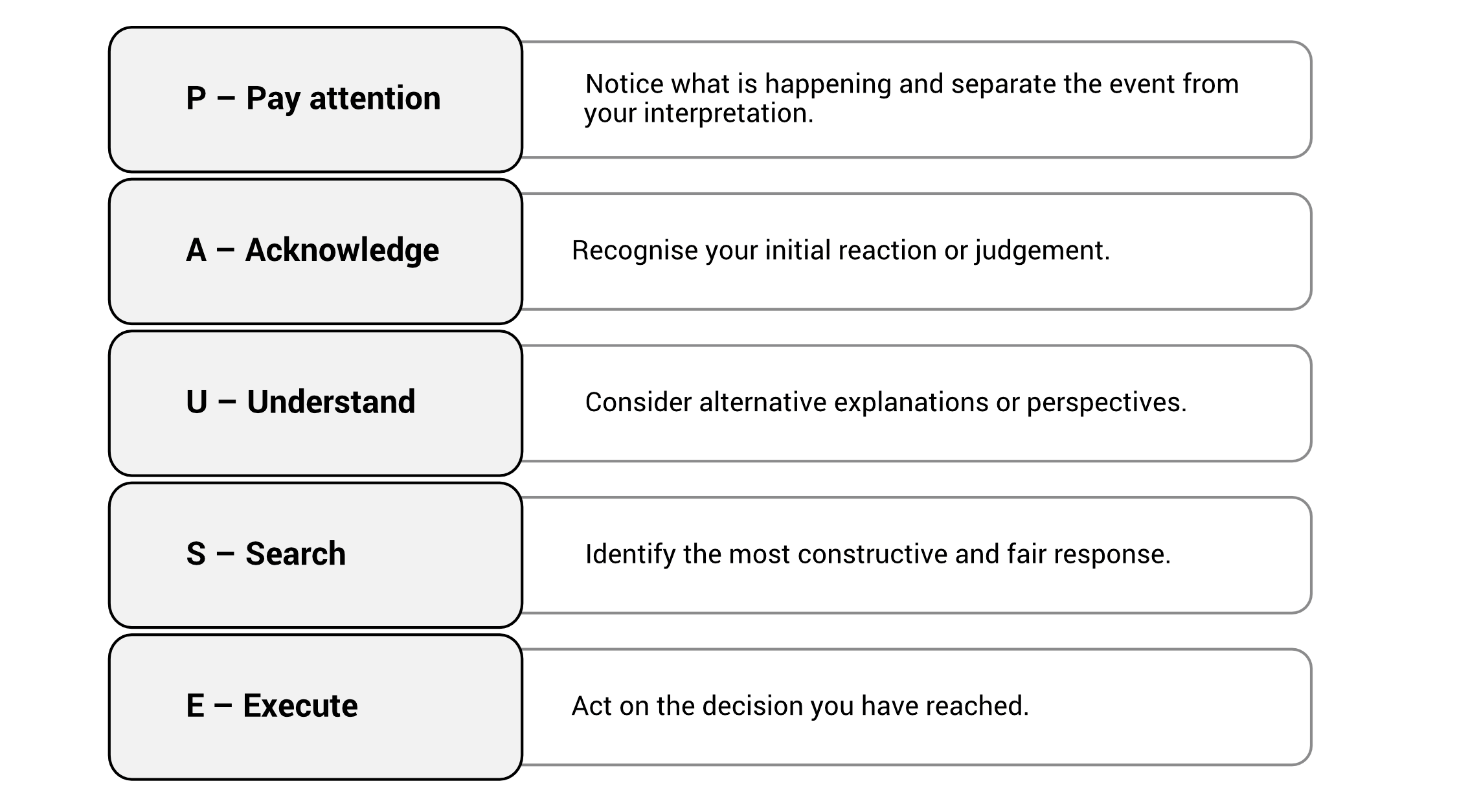
One practical framework is the PAUSE approach (NHS Midlands Leadership Academy – unconscious bias toolkit):
Building inclusive working relationships
Inclusive cultures are built through consistent, practical choices. Everyday interactions play an important role in shaping whether colleagues feel respected, valued and included. Small behaviours can influence how people experience the workplace over time.
Helpful approaches include (NHS Midlands Leadership Academy – unconscious bias toolkit):
- Showing interest in colleagues’ perspectives, acknowledging contributions, and sharing information and opportunities openly and fairly.
- Using clear and respectful communication: listening carefully, maintaining open body language and responding in a considered way to support people feeling heard.
- Recognising and including differences in perspective, background and experience to strengthen teamwork, support balanced decision-making and improve problem-solving.
- Taking practical steps to share opportunities more evenly – for example, rotating teaching, presentations or leadership roles, and ensuring key information is communicated consistently.
- Being mindful of how informal practices and social activities are organised so they do not inadvertently exclude members of the team – for example, events centred around alcohol, or events scheduled at times that may not be accessible for those with caring responsibilities.
Reducing bias in recruitment and career development
Clear and consistent processes can help reduce the influence of bias in recruitment, promotion and career development decisions. When expectations and criteria are defined in advance, decisions are more likely to be based on skills and experience, rather than personal impressions. Helpful strategies include:
- Removing identifying characteristics such as name, gender or age from early stages of recruitment.
- Using clear competency-based criteria for shortlisting, promotion and performance evaluation.
- Structured interviews where candidates are asked the same core questions and assessed using consistent criteria.
- Removing biased language from job descriptions and recruitment materials; replacing terms such as ‘native English speaker’ with ‘excellent communication skills and fluency in English’.
- Using diverse interview panels and enabling candidates to interact with a range of staff during the recruitment process. Monitoring the diversity of panels can also help organisations identify potential gaps.
- Taking sufficient time with recruitment and development decisions, and avoiding rushed judgements.
(BMJ Leader 2023;7:314, NHS Midlands Leadership Academy – unconscious bias toolkit)
Organisational approaches to tackling bias
Addressing bias requires both individual awareness and organisational action. Organisations can reduce bias by strengthening leadership, accountability and fair decision-making processes. Helpful approaches include:
- Ensuring leadership reflects the diversity of the workforce and population served.
- Holding senior leaders accountable for progress on equity and inclusion.
- Considering equity when developing policies and making organisational decisions.
- Collecting and reviewing data on recruitment, promotion, pay and disciplinary processes to identify inequalities.
- Supporting mentorship and career development for under-represented groups.
Workplace culture plays an important role. Inclusive leadership and supportive working environments help create psychological safety, allowing staff to raise concerns, challenge assumptions and contribute fully within teams. Measures that support this include:
- Protecting staff who raise concerns or report discrimination.
- Providing training on bias, cultural competence and discrimination.
- Offering flexible working arrangements that support retention and career progression.
- Supporting internationally-recruited staff and recognising their contribution to the NHS workforce.
National leadership and oversight also influence how effectively organisations address bias. Recommended measures include clearer leadership standards, national development programmes for healthcare leaders, and stronger monitoring of equality and fairness across organisations. These steps help ensure that efforts to reduce bias are implemented consistently across the health system.
(BMJ 2025:390:r1334; Future Health J 2021;8:40)
Reducing bias is an ongoing piece of work, rather than something solved by a single policy or training session. It involves staying aware of our own assumptions, taking time over important decisions, using fair processes in areas such as recruitment and progression, and paying attention to how people are treated in everyday working relationships. These efforts also depend on having the time and conditions that allow people to think carefully, rather than rushing decisions. Over time, these small but consistent actions can help build workplaces where people feel respected, supported and able to work well together.
|
Bias in healthcare
|
|
| Explore your own implicit biases around a wide range of factors, including weight, skin colour, gender and disability, through Project Implicit at the University of Virginia. These are best used as tools for reflection and learning, rather than definitive measures of personal bias. | |
|
Useful resources: Websites (all resources are hyperlinked for ease of use in Red Whale Knowledge) Videos |
This information is for use by clinicians for individual educational purposes, and should be used only within the context of the scope of your personal practice. It should not be shared or used for commercial purposes. If you wish to use our content for group or commercial purposes, you must contact us at sales@red-whale.co.uk to discuss licensing, otherwise you may be infringing our intellectual property rights.
Although we make reasonable efforts to update and check the information in our content is accurate at the date of publication or presentation, we make no representations, warranties or guarantees, whether express or implied, that the information in our products is accurate, complete or up to date.
This content is, of necessity, of a brief and general nature, and this should not replace your own good clinical judgment or be regarded as a substitute for taking professional advice in appropriate circumstances. In particular, check drug doses, side effects and interactions with the British National Formulary. Save insofar as any such liability cannot be excluded at law, we do not accept any liability for loss of any type caused by reliance on the information in these pages.
Here is the link to our terms of use.